ANXIETY AS A PREDICTOR OF GLOBAL FUNCTIONING IN A SAMPLE OF PATIENTS DIAGNOSED WITH SCHIZOPHRENIA AND SCHIZOAFFECTIVE DISORDER
Abstract
Background:Co-morbid anxiety accelerates the already existing impairment in daily functioning of schizophrenic p a t i e n t s , w i t h n e g a t i v e i n t e r f e r e n c e o n t h e outcome.Objectives:The study aims to determine if anxiety can be used as a predictive factor for the global functioning of patients with schizophrenia/schizoaffective d i s o r d e r , u n d e r a n t i p s y c h o t i c treatment.Methods:Considering the treatment,study e n r o l l e d 3 9 p a t i e n t s , d i v i d e d i n t w o groups(1.olanzapine,quetiapine,with some efficacy on anxiety,and 2. haloperidol,risperidone,aripiprazole,less efficient on comorbid anxious symptoms).The 2 groups were formed of hospitalized schizophrenic and schizoaffective disorder patients,according to DSM- 5,ICD-10 criteria.All participants were evaluated with psychological and clinical scales;PANSS,HAM-A,HAM- D,GAF,from baseline(admission),to 6 months after discharge.Results:In this study,both types of treatments presented similar degree of efficacy in reducing psychotic and affective symptoms(anxiety,depressive,mania).In HRA group,anxiety and functionality,presented stronger r e s o l u t i o n o f s y m p t o m a t o l o g y, w i t h p o s i t i v e outcome.Conclusions:The antipsychotic treatment was considered efficient but only in HRA group,anxiety can be regarded as apredictor of global functioning,especially at 3 months after antipsychotic treatment.Functionality can be influenced by antipsychotics,depending on the time of administration.
INTRODUCTION
Schizophrenia is a severe mental illness that often co-occurs with anxiety and can be exacerbated by other psychiatric conditions.Prevalence estimates are influenced by heterogeneity among definitions of symptoms and rating instruments used for diagnosis.Other diagnostic issues complicating the study of anxiety in s c h i z o p h r e n i a a r e t h a t s y m p t o m s m a y o c c u r spontaneously,intermittently,as a indirect response to psychotic symptoms or may be considered a side effect of antipsychotic medications.
It is know that co-morbid anxiety can negatively impact the outcome of schizophrenic patients by reducing global functioning.
I n a l o n g i t u d i n a l s t u d y p e r f o r m e d o n schizophrenic and schizoaffective disorder patients, hospitalised in Psychiatry Department of Emergency County Clinic of Arad,we intented to determine in what way co-morbid anxiety impacts functionality for these patients.
OBJECTIVES
The main goal of the present 6 months longitudinal study was to determine whether the co- occurence of anxiety can predict global functioning of schizophrenic and schizoaffective disorder patients.To accomplish that,pending on administrated antipsychotic’s (1.olanzapine/quetiapine,know to have positive effect on anxiety or 2.haloperidol /risperidone /aripiprazole,with lower interference with anxiety),first we have analyzed the relationship between anxiety,schizophrenia and schizoaffective disorder.Second,the efficiency of study antipsychotic treatment in reducing affective symptoms (anxiety,mania,depression)was evaluated.Third,the d i f f e r e n c e s i n e f f i c i e n c y o f t r e a t m e n t t y p e s (1.olanzapine,quetiapine and 2.haloperidol, risperidone, aripiparazole) and the severity of co-morbid anxiety on psychotic symptoms was assessed.
PROCEDURE AND DESIGN
1. METHOD
The study was approved by the Ethics Commision Board of Emergency County Hospital of Arad,”Vasile Goldis”Western University”Vasile Goldis”of A r a d , i n c o n f o r m i t y w i t h t h e D e c l a r a t i o n o f Helsinki(1).Prior to any study procedures,all participants consented to take part in the study.Assessments were performed by researchers in Psychiatry Department of Emergency County Clinic of Arad,on 4 evaluation p o i n t s : a d m i s s i o n ( T 1 ) a n d a f t e r d i s c h a r g e , a t 2 8 days(T2),3months(T3),and 6 months(T4).Psychological and clinical scales (PANSS(2),HAM–A(3),HAM- D(4),YMRS(5),GAF(6)were applied.Antipsychotic treatment and dosage was established by treating psychiatrist.A statistical analysis was conducted:Repeated Measures,t Test,Multivariate Anova(7).Partial correlation for each group(considering the diagnosis as control variable)was used to achieve the first objective.For the second objective,we applied an experimental design with repeated measurements,firstly,to verify the base level of each variable in each analyzed group,in order to test for independent samples and secondly,Reapeted ANOVA.The third objective was determined through statistical control of psychosocial variables(HAM-A scores)at admission (T1)and Multivariate ANOVA for(T2,T3,T4).
Initially,the sample included 57 inpatients recruited between 2014-2015 from Psychiatry D e p a r t m e n t o f E m e rg e n c y C o u n t y C l i n i c o f Arad,diagnosed with schizophrenia/schizoaffective d i s o r d e r, a c c o r d i n g t o D S M – 5 – T M ( 8 ) , I C D – 1 0 ( 9 ) criteria.After baseline evaluation,only 39 inpatients met the inclusion criteria:(A)documented diagnosis of schizophrenia/schizoaffective disorder,with co-morbid anxiety,(B)age between 18 and under 65 years old,(C)no other psychiatric or somatic co-morbidities,(D)no history of refractory schizophrenia.The exclusion criteria were:(A)first psychotic episode,(B)lack of co-morbid a n x i e t y, ( C ) a g e u n d e r 1 8 o r a b o v e 6 5 y e a r s old,(D)associated somatic or psychiatric pathology, (E)history of treatment resistant psychosis.
2. INSTRUMENTS
Co-morbid psychiatric disorders(anxiety) were s c r e e n e d b y u s i n g t h e M i n i I n t e r n a t i o n a l Neuropsychiatric Interview (M.I.N.I.6.0)(10).Defined anxiety was assessed using Hamilton Anxiety Rating Scale (HAM-A)(3),(scores greater than 8).Depression was identified using Hamilton Depression Rating Scale(HAM-D),(4)scores greater than 8.The presence of manic symptoms was defined by scores greater than 8 on the Young Ziegler Mania Rating Scale (YMRS) (5).Overall functioning was assessed using the Global Assessment of Functioning Scale (GAF) (6).Additionall information regarding age, sex, educational level,lifetime history of psychosis,number of illness episodes,income was collected.Final enrollement captured a total of 39 hospitalised patients (26schizophrenics and 13 schizoaffective disorder),age between 29 and 58 years(m=41.66;SD=7.31),23 females(59%)and 16 males(41%),divided in two relatively homogeneous groups,OQ(N=18)and HRA(N=21),as presented in Table1.
3.RESULTS
A specific statistical analysis concerned differences between females and males in each group (OQ and HRA) at phase T1 (admission) for each scale and subscale,did not reveal significant differences between groups (p>.05;d=NS),indicating the homogeneity of groups as far as gender concerns (Table2).
By comparing the two treatment groups(t test for independent samples),the result revealed no statistical significance for the severity of psychosis(PANSS scores),anxiety(HAM-A),depression(HAM-D)and mania(YMRS)among groups(Table 2).We can only observe that patients enrolled in haloperidol, risperidone,aripiprazole group presented predominantly positive psychotic symptoms(PANSS-P(T1)[t(37)=- 4,374;p<.001;d=1.40];size effect 91,9%). Longitudinal measures(Repeated ANOVA) evaluated antipsychotic’s efficacy in reducing a n x i e t y, f r o m a d m i s s i o n u n t i l s i x m o n t h s o f treatment(Table3).Anxiety was reduced in both groups:OQ[F(3.17)=17,018;p<.001;η=.50]and HRA group [F(3.20)=20,273;p<.001;η=.50].Some differences must be mention at six months evaluation in group HRA,were we noticed a pronounce decrease for anxiety [t(37)=2,257;p=.03; d=.73],as supported by a variation of 76% from the data dispersion value (see Table 3).
Depressive symptoms(Repeated ANOVA for HAM-D)tended to improve,suggesting a relatively similar level of antypsychotic’s efficacy in both g r o u p s : ( T 2 ) [ t ( 3 7 ) = 1 . 4 8 5 ; p = . 1 4 ] ; ( T 3 ) [ t ( 3 7 ) = 1 . 1 6 1 ; p = . 2 5 ] ; [ t ( 3 7 ) = 0 , 5 2 8 ; p = . 6 0 ] , ( Ta b l e3).Manic symptoms assessements(Repeated Anova for YMRS)showed that antipsychotic treatment had a high degree of efficacy and improved the extent of self- reported manic symptoms,with no major statistical significance among groups:T2[t(37)=0.559;p=.57],T3 [t(37)=-0.118;p=.90] and T4 [t(37)=-0.086;p=.93],(Table4).
Final comparison between groups(OQ,HRA)in postreatment phases(T2,T3,T4)failed to show noticeable differences in treatment superiority: T2[t(37)=1.613; p = . 1 1 ] ; T 3 [ t ( 3 7 ) = 1 . 1 9 2 ; p = . 2 4 ] ; a n d T 4 [t(37)=1.855;p=.07].
3.PREDICTORS OF GLOBAL FUNCTIONING IN STUDY SAMPLE
Preliminary analysis(multi-linear regression), p e r f o r m e d i n o r d e r t o p r e d i c t h o w g l o b a l functioning(GAF)might be influenced by anxiety(HAM- A)in posttreatment phases(T2, T3,T4),allow us to believe that anxiety assessed at 28 days,3months and 6 months after antipsychotic treatment,may be an important predictor for estimating functionality in patients diagnosed with schizophrenia,schizoaffective disorder (Table 5).
Considering anxiety as predictor,in Table 5,we noticed the statistical variations among estimated measures on regression equation by comparison with the mean results for the two study samples:patients treated with olanzapine, quetiapine [F(3.17)=.012;p=.99] and for those treated with haloperidol,risperidone, aripiprazole [F(3.20)=3.728;p<.03].
M u l t i p l e C o e ff i c i e n t o f D e t e r m i n a t i o n (11),representing a percentage of global functionality dispersion,was explained by the common action of p r e d i c t o r s ( H A M – A a t T 2 , T 3 , T 4 ) . T h e M u l t i p l e
Coefficient of Determination for OQ group was R2=.003, suggesting that in these group,predictors(anxiety assessed at T2,T3,T4)presented a 0.3% contribution of global functioning dispersion.In the HRA group,the Multiple Coefficient of Determination was R2=.397 (indicating that predictors contributed for 39.7% of global functionality dispersion).
Applying t test for independent samples,we obtained statistical significance data for estimating the g l o b a l f u n c t i o n i n g f o r H R A g r o u p . I n t h e s e group,considering anxiety as predictor at 28 days(B=-
.23)and 6 months of treatment (B=-2.15),we observed a negative indirect relationship between anxiety and global functioning (GAF).In contrast,HAM –A predictor at 3 months after treatment presented a direct correlation with global functioning (B=1.69).
For the HRA group,HAM-A predictors at T3 (β=1.31; t=3.276; p<.004) and T4evaluation points (β=- 1,22;t=-3.045;p<.007),were highly involved in global functioning of psychotic patients,but HAM-A at T3 evaluation point may be consider the most significant predictor,as it had the highest β value (Table 5).
The semipartial correlation(rsp) for anxiety, assessed at 3 months,with global functioning, was rsp=.61 and the coefficient of determination for the relation was 37,21%(.642; .3721,) indicating a powerfull effect on functionality,similar to anxiety at 6 months(rsp=.57;.3249).For anxiety at 28 days,the semipartial correlation (rsp=.17)had a low impact on global functioning of only 2.89%.Resuming,for HRA group,the three predictors(HAM-A at T2,T3andT4) had a strong cumulative effect R2 =.397 (39.7%)in explaining dispersion on global functioning.
Looking at the data for the OQ group, we noticed that the cumulative effect of HAM-A predictors at T2,T2 and T4,registred a low value(R2=.003;0.3%)with no impact on patients functioning.
DISCUSSIONS AND CONCLUSIONS
Although study groups were homogeneous as far as gender concerned,some initial differences regarding PANSS values should be mentioned.In HRA group,we encountered pronounced positive symptoms compared to the QO group.We are incline to assume that the HRA group was formed by productive schizophrenic type,witch could have influenced the outcome and providing a higher degree of individual functionality(along with the lack any reported drug abuse or family history of illness).
When analysing the efficacy of antipsychotic treatment,we may conclude that both treatment types were efficient,with some distinctive features:in the OQ group,anxiety was significantly reduced between admission and 3 months, followed by a tendency to stability(from 3 to 6 months).Althought,in the HRA group, anxiety diminishes dramatically after admission to 28 days after antipsychotic treatment,then reacheas a high peak at 3 months,followed by a decrease at 6 months evaluation time,allowing us to conclude that anxiety is significantly reduced in the HRA group.These findings,inconclusive to others(12,13),can be misleading a n d d e m o n s t r a t e t h a t i n t h e l o n g term,olanzapine,quetiapine,provide a greater degree of efficiency in reducing anxiety in schizophrenic patients(by assuring stability of remitted anxious symptoms).All together,these determination can present great importance in treatment management of schizophrenic/schizoaffective disorder patients,as the treatment needs to be prompt and appropriately,in order to ensure safe,stable recovery and increase the chance of quality functioning.Concordant to others(14,15,16),both types of antipsychotics are efficient in reducing depression,manic symptoms and psychosis,without noticeable variation between the groups.
Functioning impairment in schizophrenia with poorer performance in social and occupational areas,remains of great interest.Analysing global functioning as determined by GAF scale,we observed that anxiety in phases T2, T3 and T4 is an important predictor for estimating functionality in HRA groups.For HRA group,anxiety evaluated at 3 months after treatment,can be used as a predictive factor for the functional outcome of schizophrenic patients.In the OQ group,global functioning was not improved after antipsychotic treatment.Although contrary to other studies(17,18,19),these results,with functional and prognostic importance,may be relevant for treatment choice.
The authors are aware of the study’s limitations:(a)missing control group,(b)study design,with
small sample size,(c)some deficiencies in the applied scales(not especially designed for schizophrenia spectrum),and due to this facts,study results may be influenced.
ACKNOWLEDGEMENT: All the authors had an equal contribution and have similar rights. All the authors approved the final version of this article.
DISCLOSURES: The authors report no conflict of interest for this article.
LIST OF ABBREVIATIONS:
1.DSM-V-TR – Diagnostic and Statistical Manual of Mental Disorder
2.ICD-10- International Classification of Diseases
3.PANSS- Positive and Negative Syndrome Scale
4.M.I.N.I 6.O-International Neuropsychiatric Interview
5.HAM-A-Hamilton Anxiety Rating Scale
6.HAM-D-Hamilton Rating Scale for Depression
7.YRMS- Young Mania Rating Scale
8.GAF- Global Assessment of Functioning
9.OQ-Olanzapine, Quetiapine Group
10.HRA-Haloperidol,Risperidone,Aripiprazol Group
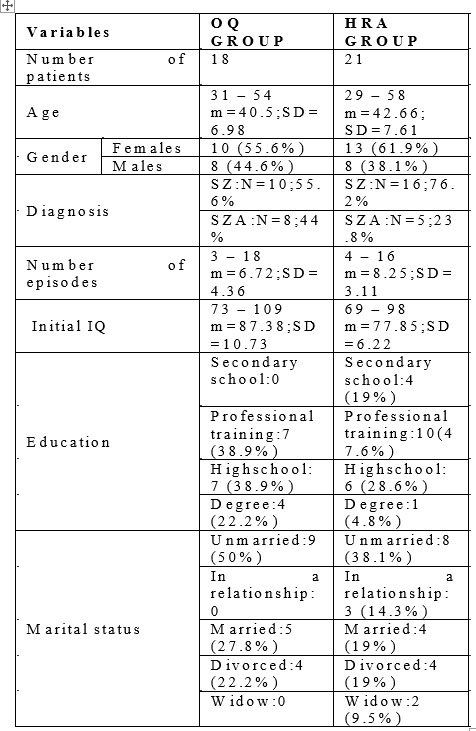
Table 1. Summary of demographic and clinical characteristics for OQ and HRA group
Note:SZ:patients diagnosed with schizophrenia;SZA:patients diagnosed with schizoaffective disorder; m:mean measurements; SD:standard deviation.
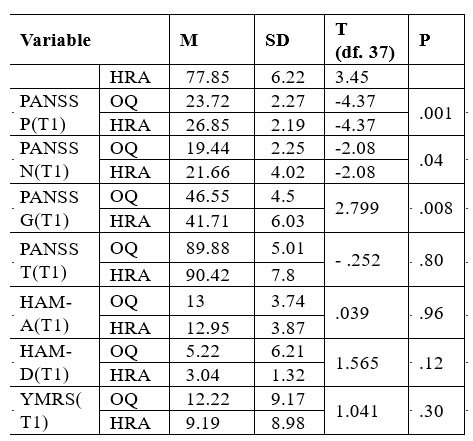
Table 2. Comparison at T1 phase (admission) of OQ and HRA groups (t test for independent samples)
N o t e 1 : O Q ( p a t i e n t s t r e a t e d w i t h o l a n z a p i n e a n d quetiapine);HRA(patients treated with haloperidol, risperidone and aripiprazol);T1- initial evaluation on admission.
Note2: df –difference *p<.05; **p<.01; ***p<.001; d –size effect.
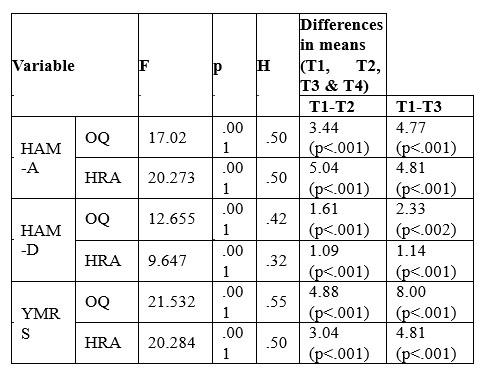
Table 3. Longitudinal changes in clinical measurements
N o t e 1 : O Q ( p a t i e n t s t r e a t e d w i t h o l a n z a p i n e a n d quetiapine);HRA(patients treated with haloperidol, risperidone and aripiprazol); T1 –at admission;T2 –at 28 days after discharge;T3-at 3 months after discharge,and T4 – at 6 months after discharge.
Note2: F= Repeated ANOVA;df –difference; *p<.001;η= size effect(0.01low;0.059 medium;0.138 high).
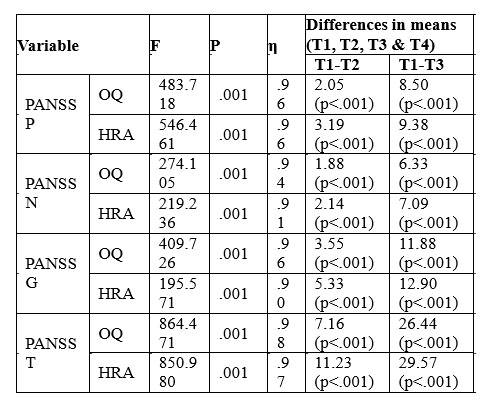
Table 4. Longitudinal changes in affective and psychotic measurements
N o t e 1 : O Q ( p a t i e n t s t r e a t e d w i t h o l a n z a p i n e a n d quetiapine);HRA(patients treated with haloperidol, risperidone and aripiprazol);T1–at admission;T2–at 28 days after discharge;T3–at 3 months after discharge;T- at 6 months after discharge.
Note2: F=Repeated ANOVA;df –difference;*p<.001;η= size effect(0.01low;0.059 medium;0.138 high).
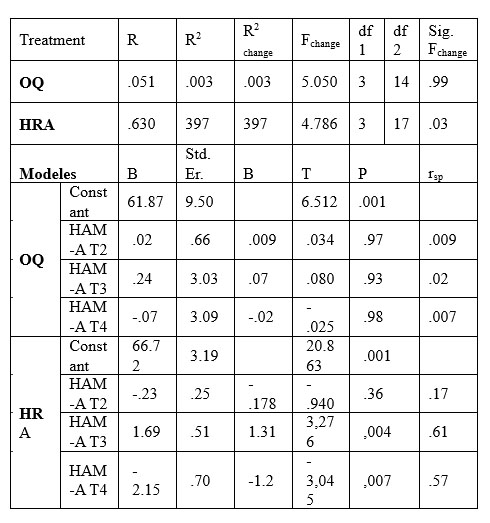
Table 5. Predictive regression equation for groups (OQ and HRA)
N o t e 1 : O Q ( p a t i e n t s t r e a t e d w i t h o l a n z a p i n e a n d quetiapine);HRA(patients treated with haloperidol,risperidone and aripiprazol);T1–at admission;T2-at 28 days after discharge;T3-at 3 months after discharge;T4-at 6 months after discharge.
N o t e 2 : R – c o e f f i c i e n t o f m u l t i p l e d e t e r m i n a t i o n ; * p < . 0 1 ; * * p < . 0 0 1 ; r s p η = s e m i p a r t i a l correlation;B–unstandardized coefficients;Std.Er.–Standard error;β –standardized coefficients;
Note3: Predictors: HAM-A at phasesT2, T3 and T4;criteria: GAF (global functionality).
REFERENCES
1.World Medical Association. WMA declaration of Helsinki: Ethical principles for medical research involving human subjects 2013 retrieved http://www.wma.et/en/30publications/10policies/b3/.
2.Kay SR, Fiszbein A, Opler LA.:The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin 1987; 13: 261- 275.
3.Hamilton M.:The assesment of anxiety states by rating. Br. J Med Psychol 1959, 32:50-55.
4.Hamilton M.:A rating scale for depression.J Neurol Neurosurg Psychiatry 1960; Hamilton Depression Rating Scale (HDRS).
5.Young RC, Biggs JT, Ziegler VE, Meyer DA. Young Mania Rating S c a l e . I n : H a n d b o o k o f P s y c h i a t r i c Measures.Washington,DC:American Psychiatric Association; 2000;540-542.
6.Hall RC.Global assessment of functioning.A modified scale. Psychosomatics.1995 May-Jun;36(3):267-75.
7.Weinfurt, Kevin P.Grimm, Laurence G.Yarnold, Paul R.,Reading and understanding MORE multivariate statistics.Washington,DC,US: American Psychological Association2000;317-361.
8.Association, American Psycyatric. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Wasington D.C.: American Psychiatric Association, 2013.
9.World Health Organization.The ICD-10 classification of mental and behavioral disorders. Diagnostic Criteria for Research Geneva,1992.
10.Sheehan DV, Lecrubier Y, Harnett-Sheehan K, Janavs J, Weiller E, Bonara LI, Keskiner A, Schinka J, Knapp E, Sheehan MF, Dunbar GC. Reliability and Validity of the M.I.N.I.International Neuropsychiatric I n t e r v i e w ( M . I . N . I . ) : A c c o r d i n g t o t h e S C I D – P. E u ro p e a n Psychiatry.1997; 12:232-241.
11.Baron, R. M., & Kenny, D. A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology,1998;1173-1182.
12.Komossa, K., Rummel-Kluge, C., Schwarz, S., Schmid, F., Hunger, H., Kissling, W., & Leucht, S.Risperidone versus other atypical antipsychotics for schizophrenia. The Cochrane Database of Systematic R e v i e w , 2 0 1 1 , D 0 0 6 6 2 6 . A d v a n c e o n l i n e p u b l i c a t i o n . http://doi.org/10.1002/14651858.CD006626.pub2.
13.Krzystanek, M. and Krupka-Matuszczyk, I.An open,large,6-month naturalistic study of outcome in schizophrenic outpatients,treated with olanzapine.Hum.Psychopharmacol.Clin.Exp.201;26: 81–85. doi: 10.1002/hup.1173.
14.Brett J. Concerns about quetiapine. Australian Prescriber. 2015;38(3):95-97. doi:10.18773/austprescr.2015.032.
15.Turkoz I, Bossie CA, Lindenmayer J-P, Schooler N, Canuso CM. Paliperidone ER and oral risperidone in patients with schizophrenia:a comparative database analysis. BMC Psychiatry.2011;11:21. doi:10.1186/1471-244X-11-21.
16.Geddes J, Freemantle N, Harrison P, Bebbington P. Atypical antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysis. BMJ : British Medical Journal. 2000;321(7273):1371-1376.
17.Nyhuis AW, Faries DE, Ascher-Svanum H, Stauffer VL, Kinon BJ. Predictors of switching antipsychotic medications in the treatment of schizophrenia. BMC Psychiatry. 2010;10:75. doi:10.1186/1471-244X- 10-75.
18.Case, M., Stauffer, V.L., Ascher-Svanum, H., Conley, R., Kapur, S., Kane, J.M., Kollack-Walker, S., Jacob, J., Kinon, B.J. The heterogeneity of antipsychotic response in the treatment of schizophrenia. Psychol. Med. 2010;DOI: http://dx.doi.org/10.1017/S0033291710001893.
19.Kinon, B.J., Noordsy, D.L., Liu-Seifert, H., Gulliver, A.H., Ascher- Svanum, H., Kollack-Walker, S.Randomized, double-blind 6-month comparison of olanzapine and quetiapine in patients with schizophrenia or schizoaffective disorder with prominent negative symptoms and poor functioning. J. Clin. Psychopharmacol. 2006;26:453–461.
***



