MONITORING ALCOHOLIC PATIENTS BY USING THE AUDIT TEST
Abstract
The purpose of the study is to identify, by applying the AUDIT test, the stages of alcoholism for patients with relapses in alcoholism. The study was carried out on a group of 331 patients diagnosed with alcoholism, which is the subject of the present paper, by using AUDIT questionnaires during all four visits, with the analysis of the dynamics of the AUDIT indicators and the dissemination of the results through the statistical methods presented in this study. The AUDIT test is a relatively easy method of diagnosis because it uses a questionnaire at the beginning of the detox period or when the patient becomes conscious. The AUDIT test is addressed to patients in both short (3 questions) and extended versions, aiming at eliminating the error rate due to patient subjectivity. Considering the psychological side and the traceability of the AUDIT test, the study aims at highlighting both the objective and the subjective values in statistically polarized data clouds according to the professional judgment of the physician and the observations collected from the biomarker analyses.
INTRODUCTION
The AUDIT test has been developed and assessed over a long period of time, and studies over the past two decades show that it provides a precise measure of the risk for alcohol consumption by gender, age and culture (1-3).
Although the AUDIT questionnaire can be applied both orally and in writing, the results may differ from one patient to another depending on how they are applied. It is advisable to provide patients with an explanation of the content of the questions, their purpose and
the need for accurate answers. The usual purpose of the AUDIT test is to determine the patient’s evolution after relapse in alcoholism. The AUDIT test can also be regarded as a pre-diagnosis for chronic alcoholism. Specialists, such as the biostatistician and alcohol abuse researcher, E.M Jellinek (4), believe that there are four phases in alcoholism. These phases are gradually being installed with the increasing intake of alcohol and the increasing frequency of alcohol ingestion. The pre- alcoholic phase, also called prodromal, corresponds to an occasional consumption of alcohol and a social need for recognition on the background of a melancholic temper or of social isolation.
The clinical stage of the disease, at this moment, does not involve physical and mental dependence, but only the need for „well-being”, which becomes manifest by the occasional consumption of alcohol. In the debut phase, the premises for the development of alcohol addiction are created. Symptoms such as amnesia, alcohol concealment, rapid first-time ingestion, feelings of guilt, or avoidance of conversation on alcoholism issues are extremely common. An important factor is the appearance of amnesia almost every time alcohol is consumed.
The critical phase is the phase in which alcohol addiction is installed, the patient experiences loss of control over the amount of alcohol he consumes and the frequency of alcohol ingestion, he becomes inebriated and intoxicated, or goes into an alcoholic coma. This is also the stage in which denial, aggressive behaviour, the persistent feeling of guilt, isolation, inactivity at the workplace, self-pity and depressive states occur, in which the patient socializes with other heavy drinkers, in which the patient consumes alcohol in the morning and neglects food and body hygiene, etc.
Once the patient reaches the chronic phase, experts / specialists believe that the patient cannot return, or will return very hard to controlled alcohol consumption. This phase coincides with the significant deterioration of the system of thinking, social relations, lack of periods of abstinence, consumption to avoid withdrawal, denial of the disease and of its effects. In severe cases, alcoholic psychoses such as alcoholic hallucinations, delirium tremens, pathological drunkenness, obsessive jealousy or Wernicke encephalopathy and Korsakov’s syndrome occur.
While the primary purpose of the AUDIT test is to identify people with hazardous or harmful alcohol consumption, researchers studying the effectiveness of the AUDIT test were also interested in using the continuity of their overall score to ensure a more rapid intervention.
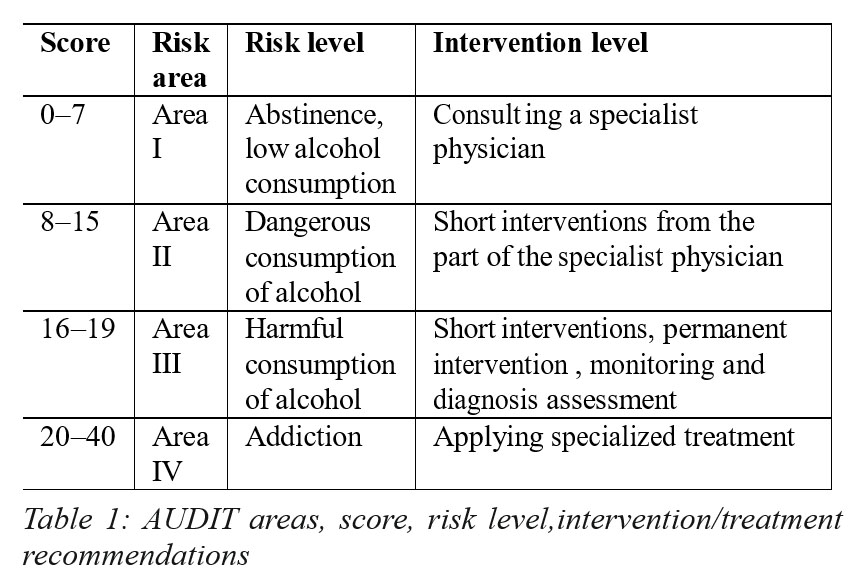
After studying the domain-related literature, we reached the conclusion that there are several areas of the AUDIT test, as well as intervention/treatment recommendations, depending on the score obtained by the patient (5).
Currently, the AUDIT test (6) is one of the most commonly used screening tools for alcohol addiction (AD) (7). It is also the alcohol screening test most often used in clinical and epidemiological research, as shown by the expansion of its application and the increase in the number of publications in the domain-specific literature. Several studies examined the psychometric properties of the AUDIT test and its ability to correctly identify people with alcohol addiction or alcohol abuse problems (AD) as defined by DSM-IV.
The monitoring of a group of patients in the African region showed, as a result of the comparison between the AUDIT test, the AUDIT-C test and the biomarker level of phosphatidylethanol, that there is a close correlation between the previously mentioned factors and alcohol consumption. The AUDIT test is thus relevant for analysing alcohol consumption (8).
These findings are also consistent with a study carried out in the emergency department of a German university hospital that found that the AUDIT test is superior in detecting alcohol abuse compared to biomarkers such as Gamma-Glutamyl-Transferase (GGT), Corpuscular Medium Volume (MCV) and Transferrin-Deficient Carbohydrates (CDT) (9).
However, a study carried out in the UK (12, 13) on parents suspected of alcohol abuse in cases investigated in child labour centres shows that, following blood tests, biomarkers of fatty acid ethyl esters (FAEE) have a longer detection period than CDT and GGT and, therefore, increased sensitivity and specificity. This FAEE Alcohol Consumption Test is correlated with AUDIT tests that show that the percentage of alcohol abusers is consistent with the percentage of blood tests (10). High concentrations of phosphatidylethanol (PE) correlate with the results obtained in the alcohol consumption AUDIT test and with the alcohol disorder consumption identification (AUDIT-C) scores. Here we refer to the application of the short version of the AUDIT test, namely AUDIT -C.
Negative EP results correlate with abstinence or alcohol consumption, so 95% of the volunteers were classified as „moderate drinkers” by the AUDIT-C test due to the e l e v a t e d p h o s p h a t i d y l e t h a n o l r e s u l t s . H i g h e r concentrations of phosphatidyl ethanol indicate excessive alcohol consumption (11, 14).
Thus, the AUDIT test remains a method of determining alcohol consumption by both adolescents and adults, along with the results of blood tests for specific and non- specific biomarkers (15).
The specialists’ concerns regarding self-assessment diagnosis tools are increasingly used in medical practice as a cheap source generating quality information. In the present paper, we aim at presenting a transformation of a classic AUDIT test model regarding alcoholism into a complex model of diagnosis based on staging alcoholic pathology.
THE DESIGN OF THE STUDY
The study is based on the screening of patients with relapses in alcoholism, the assessed people being subjected to the AUDIT test successively, during 4 detox visits. The screening procedure is the one used by the domain-specific literature – the AUDIT test, which contains a total of 10 unique-answer questions, which the authors addressed to the patients in the test group who came to four consecutive detox visits.
The objectives of the study are the following:
·Identification of the cognitive factors to which the alcoholic patient sincerely reacts and towards which he develops a sensitivity in solving the effects produced by the manifestation of the factor in the patient’s life (social- economic failure or social reintegration of the alcoholic patient).
·Identification of the factors that have a strong emotional impact on the alcoholic patient, factors that generate denial and rejection of treatment.
·Quantification of the effects of applying the AUDIT test as a screening method for classifying alcoholism into stages.
·Correlation of screening results with the evolution of the biomarker values (GGT, MCT, TB, HB, HT) in the four stages of detoxification.
From the point of view of the methods used, we applied statistical methods supported by specific informational resources (dedicated statistical programs – the GRETEL statistical program and the advantages of using the modules of the OFFICE package – the Excel and the Word modules for the systematization, processing and graphical representation of the data from the AUDIT test). The data collected after consolidation generated qualitative outcomes, quantitatively transformed by the value correspondence of the subject’s response, correspondence that the specialists made according to the impact of the response option on the general picture provided by the test.
Quantitative data, converted into average scores after all four visits, were centralized at a single average input per patient for the entire AUDIT period. The analytical (values) results were considered relative data (weights of influence), and these relative results were graphically represented by noting patient perception on each AUDIT question.
The study is a mathematical-statistical one based on the dissemination of the results obtained by applying a questionnaire / screening test on the different stages of alcoholism in the patient with relapses after detox. The methods used are data pairs, statistical observation, analytical reasoning on the relevance of the information obtained from the screening and also the representation of the data regarding the influence criteria and the impact factors of the results so that the data obtained allow conclusions, which are relevant to the purpose of the proposed research. The criteria for the selection of the test group (inclusion and exclusion criteria) were established in close relationship with the objective of the study, namely the monitoring of alcoholic patients by using the AUDIT test, the main inclusion and exclusion criteria relying on the relapse after detox, on the treatment of the disease in specialized medical units (the Psychiatry Hospital Elisabeta Doamna from Galați) and on the existence of a feedback (response / reaction) from the part of the patients regarding the questionnaire sent to be filled in (the cases in which the patients did not want to express their opinion by filling in the questionnaire were not taken into consideration).
RESULTS:
The data were collected by applying the questionnaires during each of the 4 visits and were in the database in accordance with AUDIT scoring (0-40).
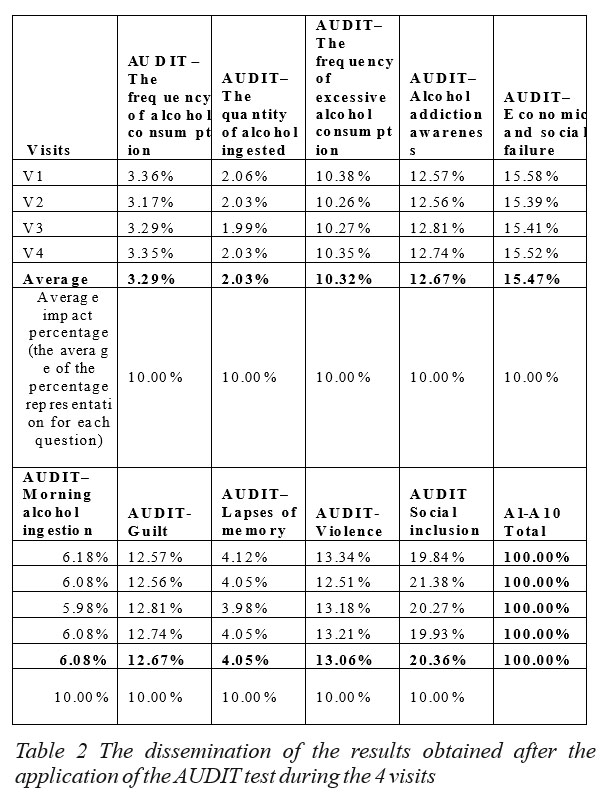
We calculated the total score/patient and the average scores recorded at each visit for the whole group of patients and for each question from the questionnaire. Afterwards, we extracted the average of the resulted scores for all the 4 visits and we applied an impact coefficient in accordance with the development stage of the disease. We calculated the total of the values obtained for each visit.
The absolute data were turned into relative data (weights), which were then transposed in a tendency that became manifest in all the visits (Table 1).
The average relative values were transformed into a general average so that we could graphically represent the patients’ cognitive perception distribution for each question from the AUDIT test. All the values were graphically transposed in Excel with the help of complex graphs, the realistic cognitive factors being separated from the subjective factors.
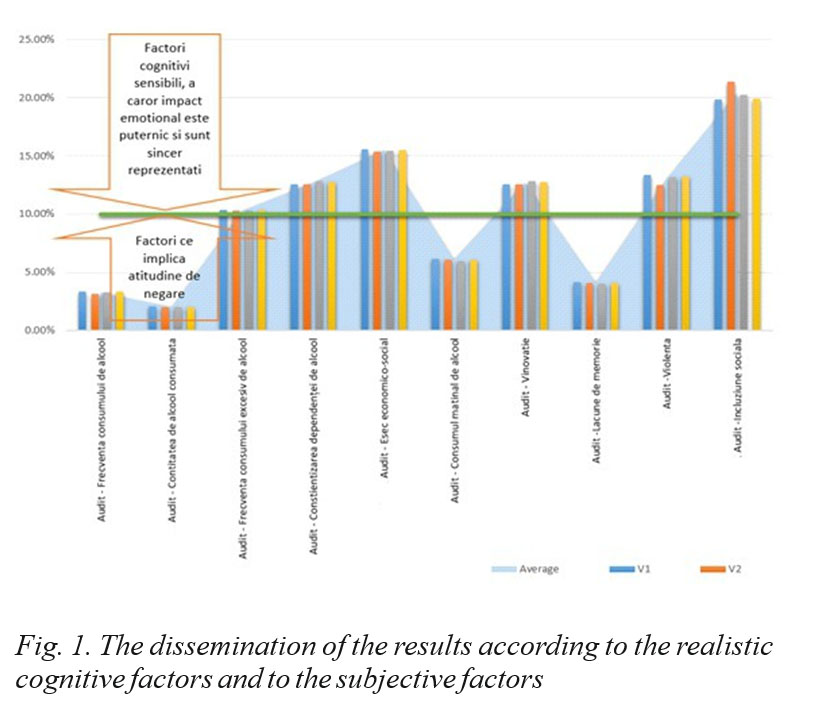
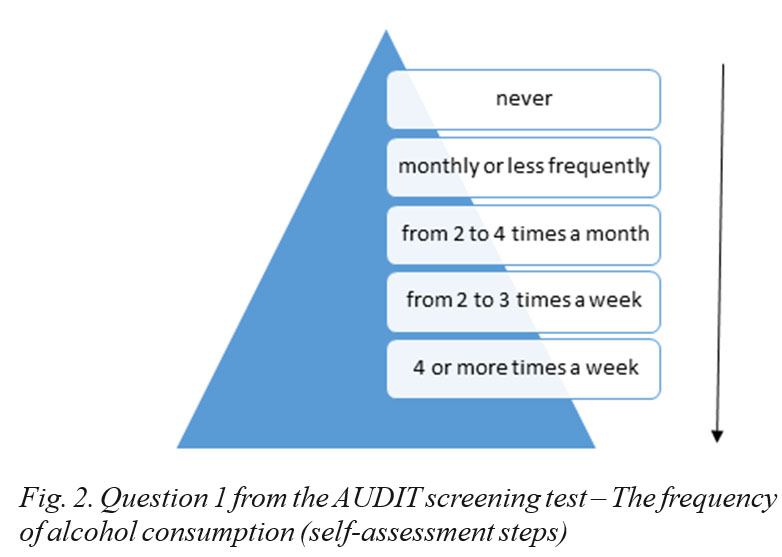
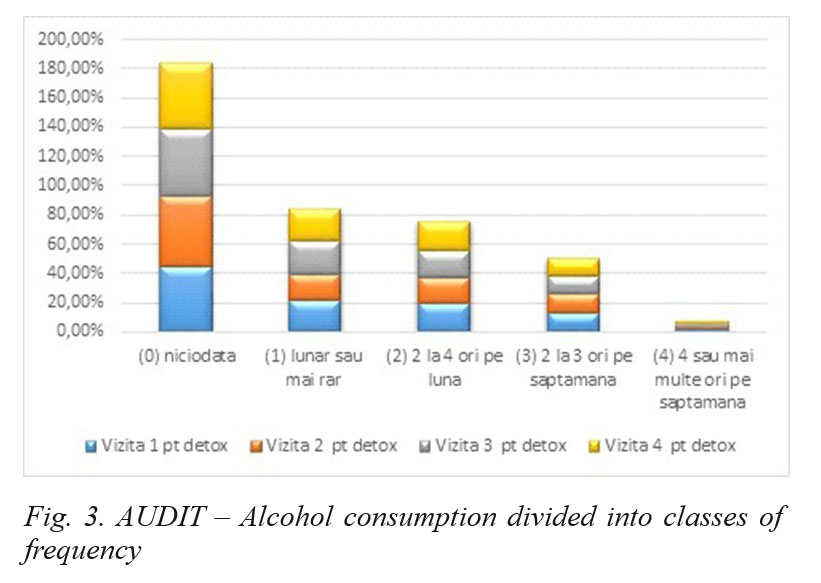
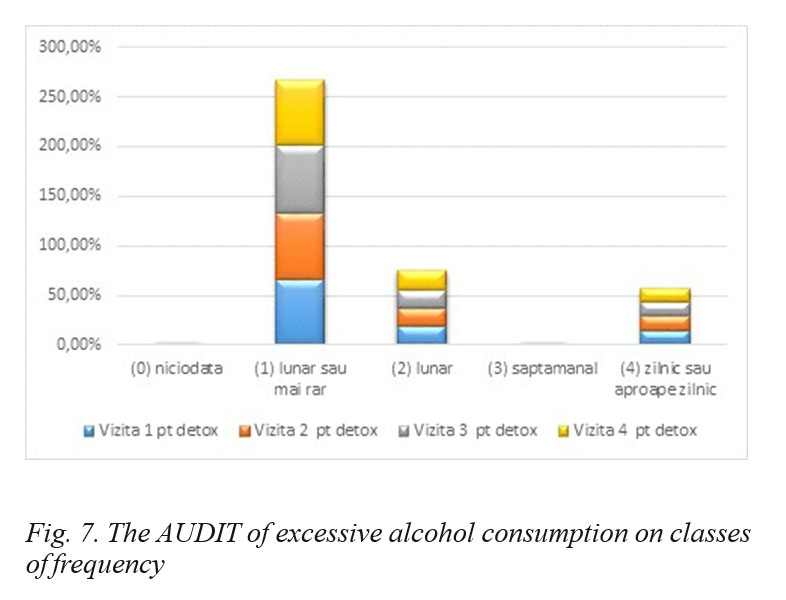
As far as the first question of the questionnaire is concerned, we may note that there is a phenomenon of denial of alcoholism among the patients, 45% to 48% of them denying alcoholism. However, we may notice the fact that, due to relapse in alcoholism, visit 2 and visit 3 for detox have the most significant rates of acceptance regarding the frequency of alcohol consumption, which occurs on the background of the psychological shock of the first detox visit.
The results are presented graphically in the figure below.
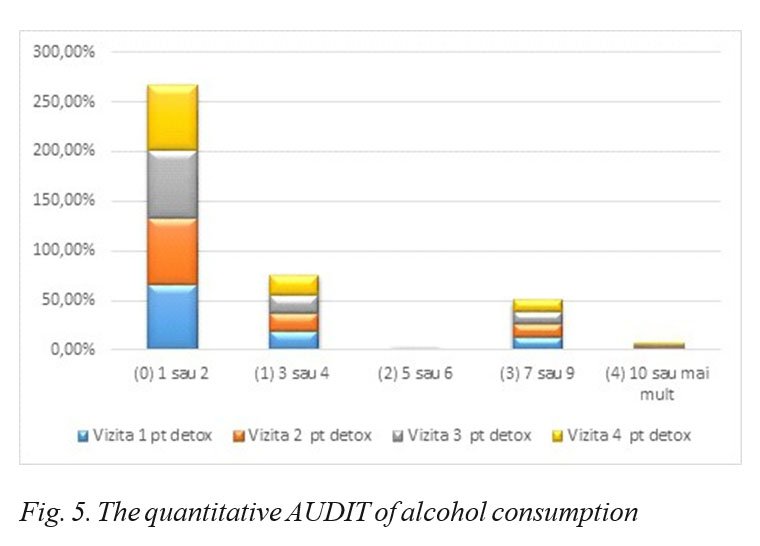
By applying question 2 from the AUDIT test, we intended to assess the awareness of the amount of alcohol consumed in relation to the GGT biomarker and to quantify the sincerity of the response in relation to the GGT analysis. The phenomenon of alcoholic denial can be observed here, by assessing the low frequency area answers (80-85%) during each visit in comparison to the critical GGT per visit between 55 and 59%, indicating that 1 out of 2 patients are not sincere in answering this question.
Following the implementation of the second question, it is clear that those who drink more shots of alcohol per day are fewer at the fourth visit but those who drink fewer shots at the fourth visit increase alcohol consumption.
This question is correctly perceived (cognitively recognized) by alcoholic patients, a number of 60 to 80% admitting the monthly consumption of alcohol and 14-
15% admitting the daily consumption of alcohol.
The above results indicate the fact that the patients accepts the disease but the coping mechanisms are not properly activated to allow the regression of the disease.
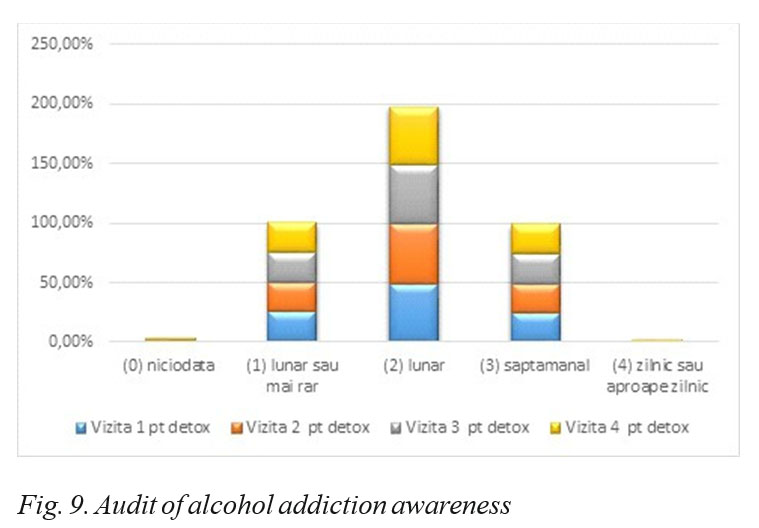
The question of alcohol addiction awareness involves a rate of sincerity above average, and patients recognize it on the background of the desire for social reintegration and the improvement in their condition, whether psychological, physical or social.
The question regarding the awareness of alcohol addiction implies a rate of sincerity above average and patients recognize it due to the desire for social reintegration and improvement in their condition, be it psychological, physical or social. For this reason, we consider that alcohol addiction is a sensitive cognitive factor, whose emotional impact is strong, being sincerely admitted by patients.
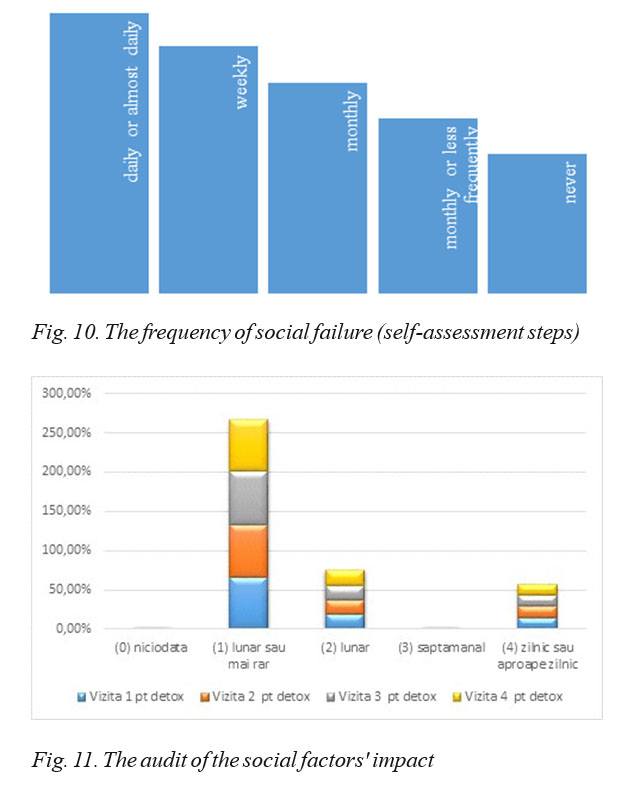
protection and social inclusion programs of people affected by alcoholism. The socio-economic failure is felt by all participating actors, namely: the patient, his/her family, local and national government bodies. The socio- economic failure is a consequence of the alcoholic crisis, which lowers the patient’s standard of living and generates great expenses from the local and national budgets, both in the health and in the economic field, by creating allowances for the support of alcoholic patients. This indicator is assessed by means of a so-called AUDIT, as a sensitive cognitive factor, sincerely admitted by alcoholic patients.
One may notice that, after the detox treatment, the percentage of patients who do not achieve what they have proposed for a short period of time is decreasing, their number decreasing as they participate in the visits; at the last visit their percentage decreases, fact which indicates the effectiveness of the treatment.
Alcohol consumption in the morning is inherent in the critical phase of alcoholism (third phase), which is a representative indicator of alcohol addiction. Like other factors, which are directly related to alcoholism, it involves a denial attitude and is poorly represented on the sincerity scale of the applied AUDIT.
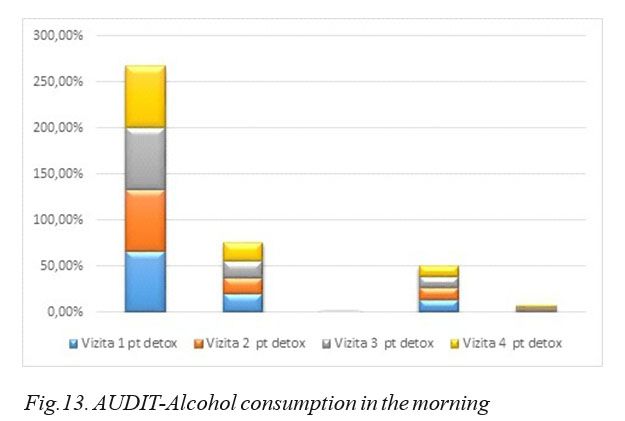
Although the vast majority of patients are confronted with alcoholism, a large percentage deny the consumption of alcohol in the morning, the percentage of those who recognize daily consumption also being very low.
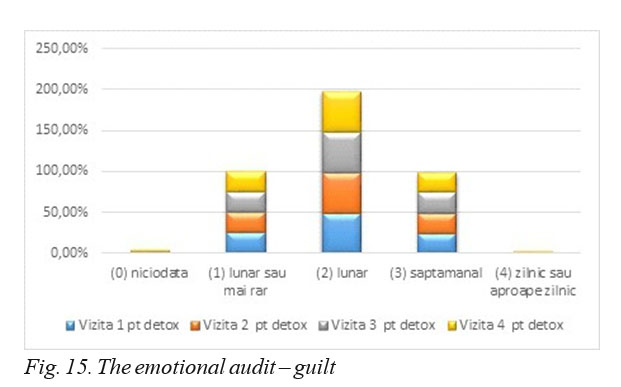
The sense of guilt is specific to the onset of alcoholism, and is recognized as a cognitive factor that is sensitive to a monthly or weekly average recognition, according to the AUDIT test performed on the 331 patients participating in the experiment, in the four detox visits.
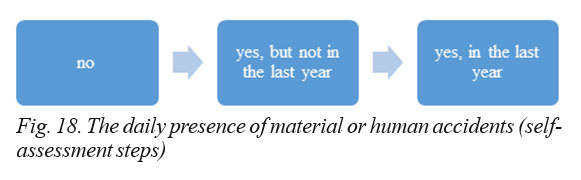
Inaccurate memory occurs in the onset of the disease and worsens as alcoholism becomes chronic. Inaccurate memory is generally denied, having a low sincerity rate from the part of the alcoholic patients, assessed by means of the AUDIT.
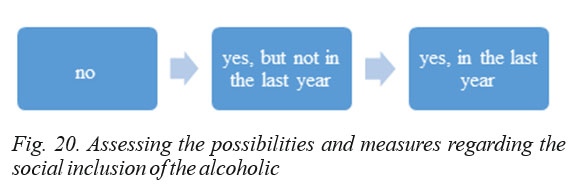
The violence associated with alcoholism from the critical stage of the disease has strong antisocial effects and causes anguish to people around alcoholics, so they adopt an attitude of avoidance and isolation of the alcoholic. Violence is generally not admitted by the family, the patient moving the frequency of violence to a longer, distant period (longer than a year). In fact, due to the specificity of the disease, people in the critical stage manifest violent acts because of emotional confusion and alcoholic jealousy
Social inclusion is quite high and assessed as such for patients with alcoholism due to the many existing programs in society, including those implemented through European funding (many people benefit from social inclusion activities or have access to national social inclusion campaigns).
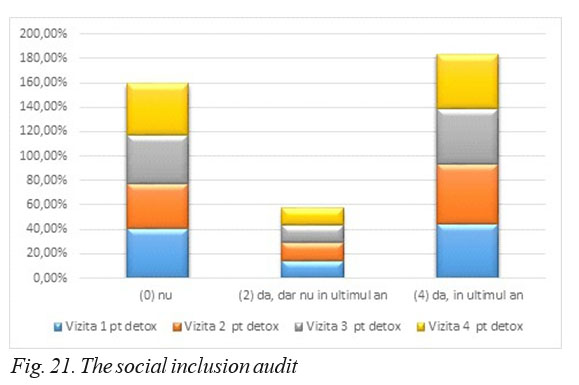
We may notice the fact that there is a relatively large number of cases in which a relative or physician has been interested in the condition of the alcoholic patient in the last year, which means that there is good communication regarding the desire for healing.
DISCUSSIONS:
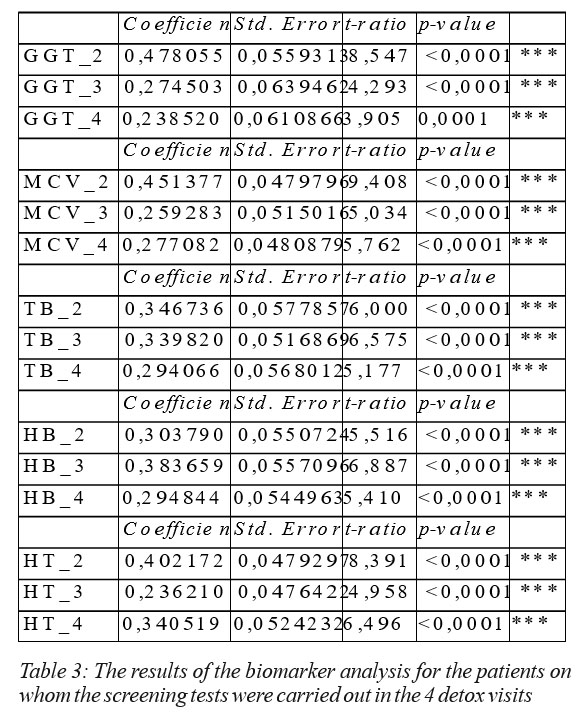
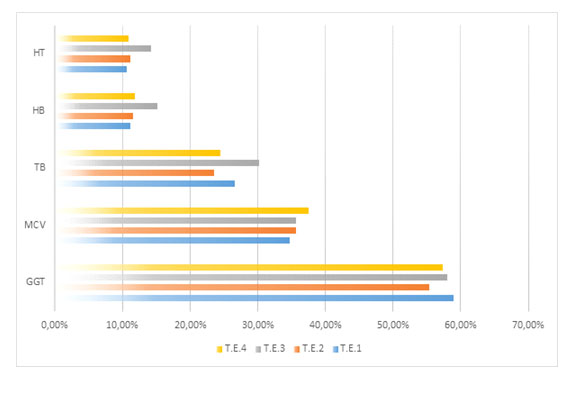
The results of the AUDIT reveal the fact that critical factors such as addiction, awareness of adverse social effects, or morning alcohol consumption are increasing during the observation period (4 consecutive DETOX visits followed by relapses in alcoholism), whereas the sensitive cognitive factors relatively improve during detox sessions. In order to assess the impact of screening in relation to traditional diagnose methods (biomarker analysis, detox pre-analysis, biochemical constant analysis (blood pressure, pulse, temperature), in the table below, we present the statistical dissemination of the biomarker analysis (GGT, MCV, TB, HB, HT) of the second detox visit and compare it to the reference period of the first detox visit.
The results of the biomarker assessments were processed by relying on the regression analysis, by means of which the distribution of the statistical phenomenon in dynamics was observed; we drew the conclusion that, within the group of 331 patients, the values have high statistical significance rates and standard errors less than 0.05. The regression coefficients, calculated in the table below in relation to the following detox visits, and compared to the first detox visit, indicate a decrease in the amplitude of the phenomenon (critical values above the standard) in the case of HB, HT and TB, fact which completes the observations from the AUDIT, which were presented above.
CONCLUSIONS:
Assessing the staging of alcoholism represents a challenge in the context of the evidence we have when the patient is first hospitalized for detox. The opportunity for appropriate staging assessment offers, from the point of view of medical practice, the possibility of a correct diagnosis and directs future clinical and paraclinical investigations and tests towards the area where they are needed.
Staging in alcoholism becomes, in this context, a filter in the application of diagnostic procedures while helping to identify patients who need psychological counseling during treatment. By means of the AUDIT screening test, applied to 331 patients, (a statistically significant group), it was possible to collect relevant observations, which were statistically analysed, and gave rise to a staging assessment model based on the transposition of the classic Audit in alcoholism model, divided on impact categories and classes of influence, in a screening model that can be applied by physicians as an instrument in the diagnosis and treatment of alcoholism in patients with relapses after detox. In order for the AUDIT to maximize its effects, the current aspects must be combined with the historical aspects, resulting in a pertinent and appropriate assessment of the status of alcoholism in the alcohol-
The audit analysis reveals the general profile of the alcoholic who is tempted to deny the disease but recognizes its effects and wants to improve or even eliminate them.
By means of the performed audit, we have identified the
applied in order to obtain the maximization of the cognitive treatment and a maximized drug support, an effort that ultimately has led to an effective control of the disease in pre-chronic stages.
The audit was designed to track the hazardous and harmful consumption of alcohol, but validity studies were
interviews such as the CIDI journal, which measures more parameters than the hazardous consumption of alcohol. Unlike screening tools, which focus on the presence of alcohol addiction or alcoholism, one benefit of the AUDIT is that it is able to identify individuals across the spectrum short-term intervention to reduce the hazardous consumption of alcohol, but also for severe alcohol consumption treatment.
Further development and improvement in the AUDIT areas may be necessary in order to allow researchers and physicians to find appropriate treatments that are more useful when choosing treatment. Further research should test empirical and gender-specific values for significant areas that reflect the severity of the addiction in people seeking treatment for alcohol-related disorders.
REFERENCES:
1. Saunders JB, Aasland OG, Babor TF, de la Fuente JR and Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. II. Addiction 1993; 88:791-804.
2. Allen JP, Litten RZ, Fertig JB, Babor T. A review of research on the Alcohol Use Disorders Identification Test (AUDIT). Alcoholism: Clinical and Experimental Research 1997 21(4): 613- 619.
3. Page P B. E. M. Jellinek and the evolution of alcohol studies: a critical essay. Addiction, 1997, 92(12): 1619-1637.
4. Babor T F, Robaina K. The Alcohol Use Disorders Identification Test (AUDIT): A review of graded severity algorithms and national adaptations, IJADR International Journal of Alcohol and Drug Research
2016, 5(2): 17 – 24.
5. Babor T F, de la Fuente J R, Saunders J, Grant M. AUDIT The Alcohol Use Disorders Identification Test: Guidelines for use in primary health care.WHO/MNH/DAT 1989; 89.
6. Selin K H. Alcohol Use Disorder Identification Test (AUDIT): What does it screen? Performance of the AUDIT against four different criteria in a Swedish population sample. Substance Use & Misuse 2006, 41(14): 1881–1899.
7. Francis J M, Weiss H A, Helander A, Kapiga S H, Changalucha J, Grosskurth H. Comparison of self-reported alcohol use with the alcohol biomarker phosphatidylethanol among young people in northern Tanzania, Drug and Alcohol Dependence 2015;156:289–296.
8. Kader R, Seedat S, Koch JR, Parry CD. A preliminary investigation of the AUDIT and DUDIT in comparison to biomarkers for alcohol and drug use among HIV-infected clinic attendees in Cape Town, Afr J Psychiatry 2012;15:346-351.
9. Schröck A, Wurst F M, Thon N, Weinmann W. Assessing phosphatidylethanol (PEth) levels reflecting different drinking habits in comparison to the alcohol use disorders identification test – C (AUDIT- C) 2017, 178: 80-86.
10. Golka K, Sondermann R, Reich S E, Wiese W. Carbohydrate- deficient transferrin (CDT) as a biomarker in persons suspected of alcohol abuse 2004 Toxicol. Lett, 151: 235-241.
11. Bush K, Kivlahan D R, Mcdonell M B , Fihn SD, Bradley K A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking, Arch. Intern. Med. 1998; 158:1789- 1795
12. Babor T F, Higgins-Biddle J, Saunders J B, & Monteiro M G. AUDIT The Alcohol Use Disorders Identification Test: Guidelines for use in primary care (2nd ed.). 2001, Geneva, Switzerland: World Health Organization.
13. Gache P, Michaud P, Landry U, Accietto C, Arfaoui S, Wenger O, & Daeppen JB. The Alcohol Use Disorders Identification Test (AUDIT) as a screening tool for excessive drinking in primary care: Reliability and validity of a French version. Alcoholism: Clinical and Experimental Research 2005; 29(11): 2001–2007.
14. Kader R, Seedat S, Koch JR, Parry CD. A preliminary investigation of the AUDIT and DUDIT in comparison to biomarkers for alcohol and drug use among HIV-infected clinic attendees in Cape Town, Afr J Psychiatry 2015; 15:346-351.
15. Joni L, Haravuori H, Lindberg N, Niemelä S, Karlsson L, Marttunen M. AUDIT and AUDIT-C as screening instruments for alcohol problem use in adolescents Drug and Alcohol Dependence 2018; 188:266-273.
***



