PATHOLOGICAL ATTACHMENT: ETIOPATHOGENIC FACTOR IN CHILD PSYCHOPATOLOGY
Abstract
Introduction: In the child's life occur traumatizing events that can change its behavior, transitory or lasting, and its mental functioning, especially if the child is younger. The child's mental vulnerability is its ability or inability to withstand environmental constraints, its ability to anticipate events and to alter the course or inability to influence them. Mother-child separation remains a traumatic event, being particularly strong in children from 5 months to 3 years. The child develops an anguished attachment reaction described by Bowlby, whose evolution and severity depends on the age of the child at the time of separation and the duration of being apart. Material and methods: 47 children were evaluated, with ages between 5.10 and 17.8 years, they were hospitalized in Pediatric Clinic of Neurology and Psychiatry in Tg.- Mures, in 2013. They were examined clinically and psychology-cally, they were applied different specific scales and questionnaires: STAI-C, MASC, scared-R, CAT, family drawing. The clinical diagnosis was established by the DSM IV-TR ICD-10. Results: Separation of mother and child is a traumatic event that modifies child behavior more so how it is smaller. Conclusions: Absence of the mother, mental illness of the biological parents, early institutiona-lization, physical or emotional neglect, physical abuse, poor socio-economic situation, the tempe-rament traits of the child constitutes an etiopathogenic factor determining: cognitive and affective disorders, psychosomatic manifestations, emotional and behavioral disorders, adaptation disorders, emphasized personality traits.
IINTRODUCTION
In the child’s psychopatology, different life events may represent risk factors for psychic diseases. “Risk factors” are all the existential conditions of the child or of the environment, that represent a risk of mental morbidity superior to the one noticed in the general population. In the child these risk factors may be: prematurity, neonatal sufferance, twins, early separations, a chronic somatic disease.
In the child’s family these risk factors may be: parental separation, chronic disagreement in the family, alcoholism, chronic disease of a parent, incomplete couple (single mother), death of one parent.
In society there are also a series of risk factors, such as: migrant situation, social and economic misery, low level of education (11).
Psychic vulnerability emphasizes the manifested or dormant sensibilities and weaknesses, immediate or postponed ones, and may be understood as an inability of the child to resist to the constraints of the environment. This may be the result of the nursling’s perception and later of the child, of his possibility to anticipate the events and to change their course through its own competence of active adjustment to the environment (1).
Affective deprivation produces variable effects depending on its nature (insufficiency, distortion, discontinuity) but also on its duration, child’s age and the mothering quality that preceded it.
The institutions that take care of nurslings have become aware of the dangers of affective mothering, making efforts to limit the number of persons who come in contact with the infant.
The need of attachment is a biological need, innate and destined for survival, constituting the premise of normal subsequent emotional development. The biological mother represents “the primordial figure of attachment”, “the primordial matrix”, ”the reassuring niche” (6). Attachment behaviors, behaviors maintaining closeness are: visual contact, smiling, watching, verbal communication, taking in one’s arms and cradling the infant (3, 10).
Maternal nursing and commitment in this process represent the early contact between infant and mother, essential in the formation of attachment. Maternal deprivation is the lack of positive mother-infant interaction, due to a multitude of causes such as: institutionalized infant, extended hospitalization, mother with physical or psychic disorders, poverty, lack of education, alcoholism, aggressiveness etc. Amidst the neglectful families there may be cases of “intrafamily hospitalism” (1, 8). These children present a range of diffuse symptomatic manifestations, noticed typically in nurslings of 5-6 months old, then in the child of 2-3 years old. In these children, it can be noted: psycho-somatic disorders and intercurrent infections: otitis, rhino- pharyngitis, vomiting, failure to thrive; some children suck their thumb with an absent, detached air, for a long time; they do not interact with the adult; psychic and language development is almost always retarded, especially language development, and the playing is poor (7, 8).
Mother-infant separation is a frequently encountered event. Bowlby, 1969 (2, 3) has described 3 stages of separation reaction: protest stage, despair stage, detachment stage (2 ,3).
This separation reaction is especially intense in the infant of 5 months old to 3 years old. Repeated separations are very harmful, the child developing an extreme sensibility and a permanent anguish, translated through an excessive dependence of his environment, described by Bowlby as “anguished attachment reaction” (3, 11). The ethiological factors involved are: psychic disorders of the biological parent (depression, psychosis) making the parent incapable of an appropriate nursing, age (very young or old parent), poor social and economic situation (physically neglected child, without clothing and appropriate food, insanitary dwelling, physical abuse etc.), frequent change and replacement of the caregiver, institutionalized child, temperamental traits of the child (too quiet child, insufferable child, etc.) (8, 9).
If separation is extended it is noticed: a frequent stopping of the affective and cognitive development; somatic disorders: decrease of immunity, falling ill frequently; psycho-somatic disorders: anorexia, nocturnal enuresis, sleep disorders; depressive symptoms; in an older child there are noticed school adjustment difficulties, learning disorders, behavior disorders (11).
The evolution depends on the age at which the separation took place and its duration (1). When affective deprivation is severe and extended, if onsets in the first year of life and persists for three years, it has very severe effects, which seem irreversible, both on the cognitive processes development of the child and on its personality development.
If affective separation and deprivation begin in the 2nd year of life, the effects on the personality development are severe, but cognitive impairment is completely reversible. Certain psychic alterations of the child are more severe and less reversible: verbal impairment, abstraction function and ability to form profound and durable interpersonal attachments.
The children’s response to a long separation from the attachment figure is manifested initially by protest, despair, subsequently by detachment, and reintroduction of the attachment figure may stir up indifference, even hostility (4, 11).
In neglected or maltreated children appear deviant forms of attachment, presenting symptoms corresponding to the 2 clinical forms: inhibited and disinhibited.
In the inhibited form appear a series of somatic and psychic symptoms. The somatic symptoms are: – decreased resistance to infections, subnutrition, nanism, retardation in psychomotor development.
The psychic symptoms encountered may be: inhibition, indifference, absence or diminished interaction capacity, hyper-vigilance, retardation in psychic development but mostly of the language (5).
In the disinhibited form the somatic symptoms encountered are: decrease of immunity and resistance to infections.
At the same time appear also a series of psychic manifestations such as: aggressiveness, emotional instability, superficial friendship relationships, aggressive behavior, hyperactivity, indifference towards the caregiver, undiscriminated sociability (7, 8).
Children with a sure attachment have better adjustment abilities, and they create coping strategies in difficult situations (7, 8).
MATERIALAND METHOD
There have been monitored during the year 2013, 47 children admitted to the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures with different psychiatric clinical diagnoses taking into account they are based on the attachment disorder. The patients have been somatically, psychically and psychologically examined, there were performed various paraclinical laboratory investigations, and applied various tests, scales and questionnaires (Raven, BDI, BECK, CAT, TAT, family drawing, STAI-C, MASC, SCARED-R, etc.) both to the child and parents. In anamnesis we monitored data related to the social and family factors, heredo-collateral factors related to the psychiatric area, the somatic, psychic and language development, sex and origin of environment. The data obtained has been represented graphically, the results have been interpreted and certain conclusions have been drawn, relating permanently to the specialized literature data.
RESULTS
In the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013, have been admitted 848 children, among which 47 have been diagnosed with Attachment Disorder according to the DSM IV-TR and ICD 10 criteria, representing 6% of the total admissions (Figure 1).
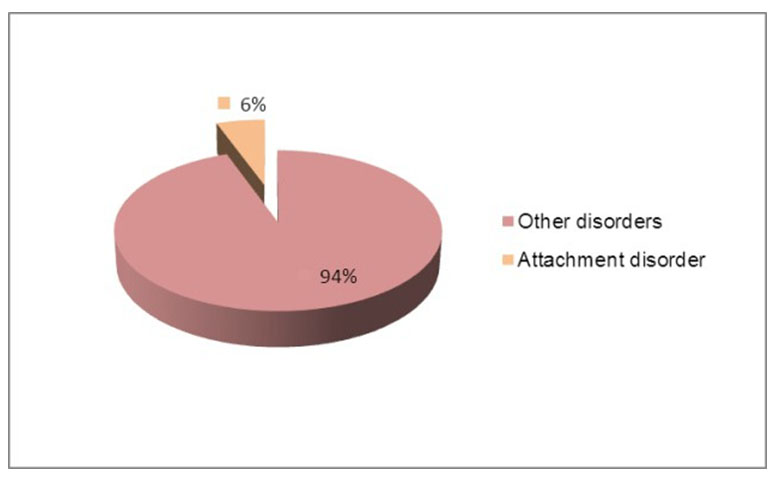
Figure 1. Admissions in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
The patients have been somatically, psychically and psychologically examined, applying also different scales and questionnaires both to children and mothers. They presented various clinical manifestations: behavioral, affective, hyperkinetic, autolytic attempts, disharmonic personality development, etc.
The age of patients was between 5,10 and 17,8 years old. Among which 12 patients (25,4%) were male and 35 (74,6%) female (Figure 2).
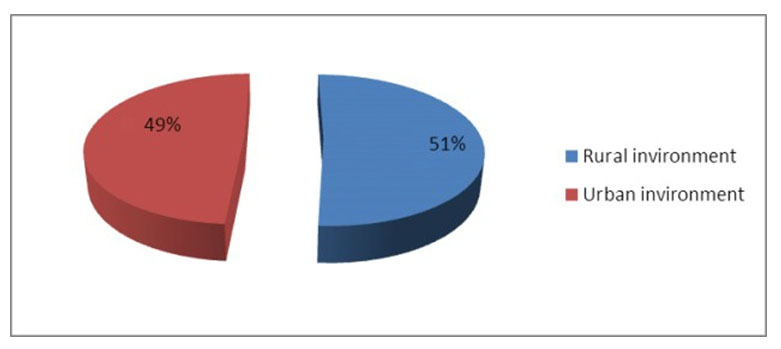
Figure 3. The environment of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
Heredo-collateral antecedents concerning the psychic pathology of the biological parents as a prone factor, were emphasized in 10 patients (21, 2%).
Thus: depression in biological parents, at 4 children (8,5%); schizophrenia: in 1 case (2,1%); personality disorders in the families of 5 children (10,6%) (Figure 4).
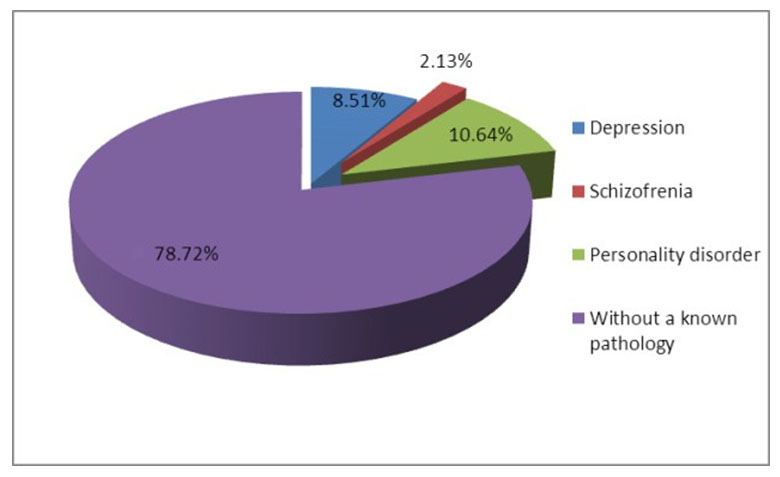
Figure 4. Heredo-collateral antecedents of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
The reasons for admission were various, consisting in: verbal impulsiveness: 22 patients (46,8%); hetero-aggressiveness: 27 patients (57,4%); self- aggressiveness: 5 patients (10,6%); sad disposition: 17 patients (36%); sleep disorders (insomnia, frequent awakenings, morning fatigue, nightmares): 10 patients (21%); decrease in school results: 18 patients (38%); school absenteeism: 8 patients (16%); hyperactivity, instability: 11 patients (22%); behavior disorders with vagrancy, theft, lie, alcohol consumption, smoking: 17 patients (36%); somatoform manifestations: cephalalgia, thirst for air, precordial pains, abdominal pains: 13 patients (26%); retardation of psychic development: 3 patients (6%); language development disorders: 5 patients (10,6%); statural and ponderal hypotrophy: 8 patients (16%) (Figure 5).
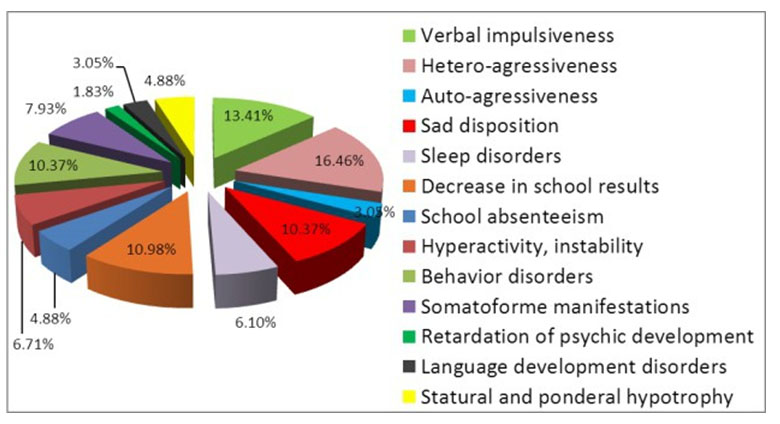
Figure 5. The reasons for admission of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
The patients have been psychologically assessed by Raven test, in order to establish the cognitive development level. Thus it has been outlined: normal intellect in 38 patients (80%); mild mental retardation in 2 patients (4%); liminality in 7 patients (15%) (Figure 6).
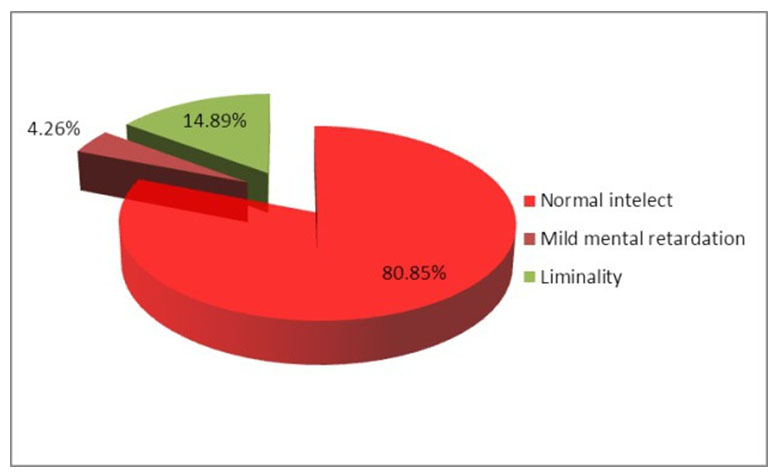
Figure 6. Cognitive development level of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
Among the social and family factors with importance in the etiology of attachment disorder, there were pointed out the following:
death of a parent: in 6 children (8.57%); child abandonment with placement in family type house or maternal assistant: in 18 cases (25.71%); extreme poverty with physical neglect: in 11 cases (15.71%); intra-family conflicts: in 13 cases (18.57%); affective neglect in family: in 7 cases (10%); alcohol consumption in family and physical abuse of the child: 15 cases (21.43%) (Figure 7).
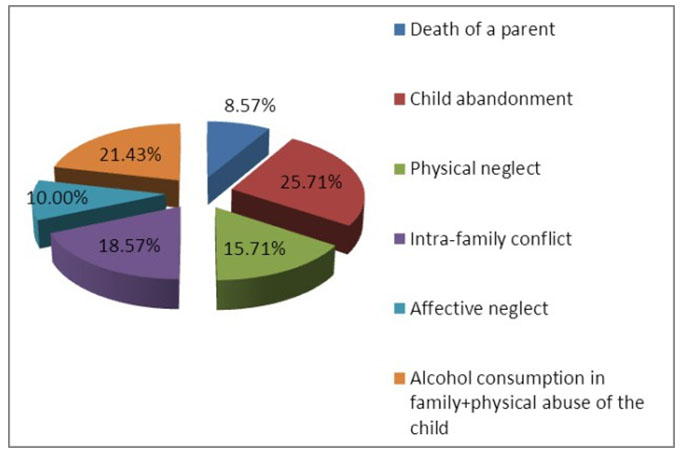
Figure 7. Family factors with importance in the etiology of attachment disorder for admission of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
For the diagnosis, in addition to the psychic examination there were applied different scales such as: STAI-C, MASC, CDI, BECK, projective tests (CAT, TAT), SCARED-R, and family drawing also. At the same time questionnaires were also used for parents. They have pointed out modifications based on which we could diagnose: ADHD: 5 cases (10,6%); anxious-depressive disorder: 8 cases (16%); socialized behavior disorder: 17 cases (36%); autolytic attempts: 7 cases (15%); disharmonic personality development: 10 cases (21%) (Figure 8).
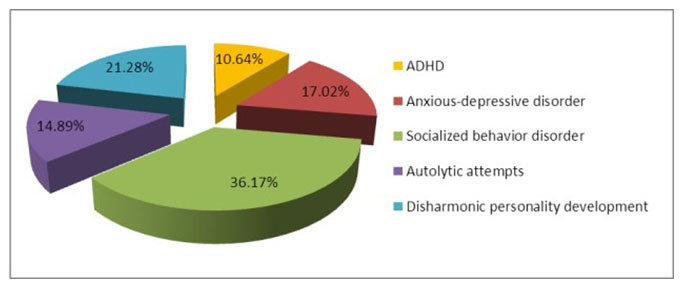
Figure 8. Diagnoses of monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
Autolytic attempts have been present in 7 patients (15%), they consisted in: voluntary medicine ingestion in 4 cases (8,5%); defenestration: 1 case (2%); veinsection in 2 cases (4%) (Figure 9).
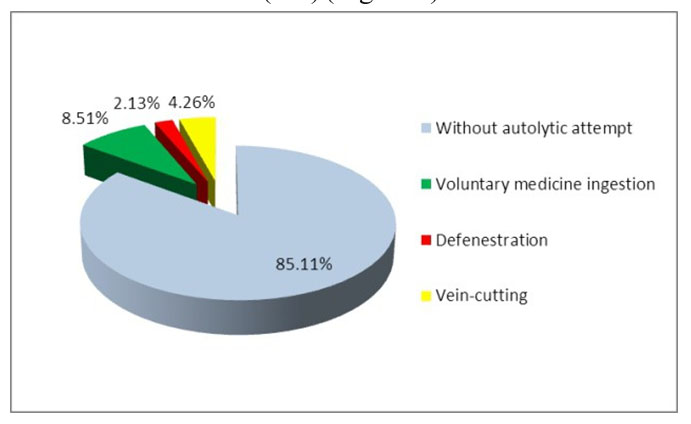
Figure 9. Autolytic attempts for monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
Disharmonic personality development has been outlined in case of 10 patients (21%); they have presented either borderline type elements (4 patients: 8,5%), or antisocial type (2 patients: 4%), or anxious-avoidant type (4 patients: 8,5%) (Figure 10).
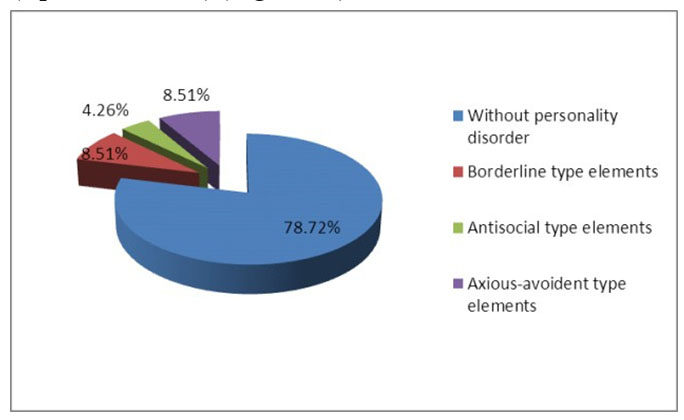
Figure 10. Disharmonic personality development at monitored children admitted in the Clinic of Pediatric Neurology and Psychiatry Tg.-Mures, in 2013
In case of a patient with Attachment Disorder and repeated autolytic attempts, with disharmonic personality development of borderline type, the family drawing has been suggestive, not representing himself in the family drawing (only the father, mother and brother) (Figure 11).
Figure 11. Case of a patient with Attachment Disorder and repeated autolytic attempts, with disharmonic personality development of borderline type
The specialized treatment of the monitored patients has consisted in anxiolytic medication (Alprazolam), antidepressants with ISSR (Sertraline), mood stabilizers (Carbamazepine, Valproic Acidum). Furthermore, it has been performed a psychological intervention consisting in family counseling, individual psychotherapy of cognitive-behavioral type. In children with retardation in psychic or language development there has been performed stimulation, in addition we used ludotherapy and drawing therapy.
In cases in which affective deprivation and neglect were emphasized, it has been disposed social and family reinsertion to maternal assistant, family type house or change of placement. At the same time it has been recommended psychiatric treatment for parents with depression or psychoses and it has been disposed the removal of the child from the natural family and his nursing by grandparents on condition that the family environment stays stable.
DISCUSSIONS
The specialized literature reminds of the fact that certain events in the child’s life may be risk factors for psychic diseases and namely: prematurity, early separations, chronic somatic disease, conflicts in family, alcoholism of biological parent, atypical families (incomplete couple: single mother), poor social and economic situation, immigrant status, low level of education (5, 11). These factors have been emphasized also in children from our trial and namely: child abandonment with placement in family type house (18 cases), poor social and economic situation (11 cases), conflicts in family (13 cases), alcohol consumption and physical abuse of the child (15 cases), affective neglect of the child by biological parent ( 7 cases).
For etiological factor in the attachment disorder there are mentioned in the specialized literature the psychic d i s o r d e r s i n b i o l o g i c a l p a r e n t s , t h e c h i l d ‘ s institutionalization with frequent change of the caregiver, biological parent’s age, either too young or too old, etc. (1, 4). In children who are in our trial, in 10 cases (21,28%) it has been emphasized the existence of the psychic disease in the biological parent and namely: depression, schizophrenia, various personality disorders.
Attachment behaviors mentioned in the specialized literature are: visual contact, smiling, infant cradling, verbal communication with the infant (3), their absence determining the apparition of the anguished attachment reaction, the child pres enting either frequent intercurrences or somatic development retardation, or psychic retardation or language development retardation, or aggressive behavior, hyperactivity, carelessness towards the family, undiscriminated socialization etc., which it has been noticed also in the patients included in our trial. The psychic functions the most severely affected in the children in our trial have been: verbal function, abstracting function, the ability to form profound and durable attachments. Affective deprivations produce variable effects on the child’s development depending on their nature, duration, child’s age and mothering quality, consisting in the retardation of the cognitive development, as well as producing effects on the child’s personality.
CONCLUSIONS
Affective deprivations (mother’s absence, psychic diseases of the biological parent incapable of an appropriate nursing, early institutionalization, affective or physical neglect, physical abuse, poor social and economic conditions, family conflicts etc.) constitute a etiopathogenic factor (RUTTER).
Reactive attachment disorder is manifested by: cognitive disorders, psycho-somatic manifestations, emotional and behavioral disorders, adjustment disorders, pronounced personality disorders.
Mother-infant separation is a psycho-traumatic event which changes the child’s behavior, all the more so as the child is younger, in the first year of life having irreversible effects on the cognitive development.
There are severely affected: the verbal function, the abstracting function, the ability to form profound and durable interpersonal attachments.
BIBLIOGRAPHY
1.Ainsworth M.D.S. The development of infant – mother attachment.
Chicago Review of child development research 1979;3.
2.Bowlby J. Attachement et perte: la separation ongoisse et colere. (Attachment and loss: separation, anguish and rage). Paris: PUF, 1978.
3.Bowlby J. Attachment and loss, Vol 1 Attachment. New York: Basic Books, 1982.
4.Cicchetti D, Cummings E.M, Greenberg M.T. An Organizational perspective on attachment beyond infancy. In: Greenberg M.T, Cichetti D, Cummings E.M. (eds). Attachment in the preschool years. Chicago: Chicago University Press, 1990.
5.Dobrescu I. Manual de psihiatria copilului si adolescentului, (Child and Adolescent Psychiatry Manual). Bucureşti : Ed. Infomedica, 2010, 229-239.
6.Izard C.E. et al. Emotional determinants of infant-mother attachment. Child development 1991, 62.
7.Kaufman I. Depressive disorders in maltreated children. J. Am. Acad. Child Adolesc. Psyhiatry 1991;30(2): 257-259.
8.Martin A., Volkmar F. Lewis’s Child and Adolescent Psychiatry. Philadelphia: Lippincott Williams and Wilkins, Fourth Edition, 2007, 711-717.
9.M a r c e l l i D . Tr a t a t d e p s i h o p a t o l o g i a c o p i l u l u i . ( C h i l d Psychopathology Treatise). Ed. Fundaţiei Generaţia, 2006, 446-474.
10.Mircea T. Tratat de psihopatologie a dezvoltarii copilului si adolescentului. (Psychopathology Treatise of Child and Adolescent Development). Timisoara: Editura ArtPress, 2006, 83-87, 337-355.
10. Rutter M, Bishop D, Pine D, Taylor E. Rutter’s Child and Adolescent Psychiatry, Fifth Edition. Blackwell Publishing, 2009, 906-913.
***


