IRRITABILITY AND PERSONALITY TRAITS AS SUICIDE RISK FACTORS IN DEPRESSION
Abstract
Introducere: Suicidul este una din principalele urgenţe psihiatrice şi o problemă importantă de sănătate publică în majoritatea ţărilor lumii. Între tulburările psihice, cel mai mare risc suicidar îl au tulburările afective. Obiectiv: Studiul prezent a evaluat impactul impulsivităţii, agresivităţii, iritabilităţii şi al toleranţei scăzute la frustrare asupra riscului suicidar în depresie. Metodă: Acest studiu a fost efectuat pe un lot de 103 pacienţi de sex masculin care au fost internaţi pentru un episod depresiv, indiferent de tulburarea afectivă diagnosticată (depresie unipolară, tulburare bipolară sau tulburare afectivă secundară unei suferinţe somatice). Pacienţii au fost evaluaţi prin interviu clinic şi scale autoadministrate. Ca variabilă rezultat a riscului suicidar a fost utilizată prezenţa internării ne-voluntare. Rezultate: Analiza statistică a datelor obţinute a relevat o corelaţie semnificativă între riscul suicidar şi impulsivitate (p<0.001), agresivitate (p=0.059) şi toleranţă scăzută la frustrare (p=0.003). Iritabilitatea (p=0.266) nu a avut o corelaţie semnificativă cu riscul suicidar, dar a fost înalt corelată cu prezenţa impulsivităţii (p<0.001) şi a agresivităţii (p<0.001). Concluzii: Studiul nostru confirmă importanţa evaluării impulsivităţii şi agresivităţii în cadrul stabilirii riscului suicidar. În privinţa iritabilităţii şi toleranţei scăzute la frustrare ca factori de risc în suicid sunt necesare studii ulterioare care să clarifice importanţa lor.
INTRODUCTION
Suicide is one of the main psychiatric emergencies and an important public health problem in most countries around the world (1). The evaluation of suicide risk is one of the core competencies a psychiatrist has to develop during his training and professional life. This evaluation is a complex problem, which involves assessing and integrating numerous risk factors. To date there is no clinical or biological instrument that can accurately predict suicide.
The presence of mental illness is one of the most important factors that increase suicide risk, being present in 90% of all suicides (2). Studies have shown that two thirds of these suicides associated with mental illness are associated with depression. Nevertheless, the great majority of people who suffer from a mental illness do not kill themselves and do not even attempt suicide. This fact led Mann et al to propose, in 1999, a diathesis model. This model comprises of two facets of the suicidal patient: a tendency to experience more suicidal ideation and a tendency to be more impulsive, therefore more likely to act on suicidal thoughts and feelings (3). Thus, these authors are among the first to raise awareness to the importance of impulsivity as a predictor of suicidal behavior. Since then there have been many studies that have taken into account impulsivity as a factor in suicide risk.
Also, completed suicide is up to three times more frequent among men, although there are more attempted suicides among women (4). This is due, at least in part, to the fact that men tend to use more lethal means in hurting themselves. For this reason the present research focuses on the suicide risk of men with depressive episodes.
Suicide risk and impulsivity have also been connected to aggression. This is both due to the fact that suicide is viewed as aggression turned inwards and to the fact that all three of these factors have been linked to serotonin regulation abnormalities (5, 6, 7).
Therefore this study aims to study the link between suicide risk and trait impulsivity and trait aggression. Another hypothesis we want to test is that the degree of irritability developed during a depressive episode is related to the overall aggression and impulsivity of the individual and whether this symptom is relevant in the evaluation of suicide risk. Also we aim to evaluate the importance of low tolerance to frustration for the suicide risk of a depressive episode.
METHOD
This study included a cohort of 103 male
inpatients. It was conducted in the 3rd Department of “Prof. Dr. Al. Obregia” Clinical Hospital of Psychiatry in Bucharest, over a period of two years. Patients with a diagnosis of Depressive Episode were included, regardless of the type of mood disorder diagnosed – unipolar depression, bipolar disorder or depressive disorder due to a general medical condition. Comorbidity (either psychiatric or somatic) was not a criteria for exclusion from the study. DSM IV-TR criteria were used to diagnose the depressive episode. As an independent outcome variable for the evaluation of suicide risk we used the type of hospitalization (either voluntary or involuntary). The involuntary hospitalization was determined by a commission composed of three professionals, according to the Romanian Mental Health Law. The study included only those patients with depressive episodes for whom the involuntary hospitalization was decided on the basis of suicide risk.
Each patient was interviewed upon admission and they also completed two self-administered questionnaires: the Barratt Impulsiveness Scale (BIS) and the Brief Aggression Questionnaire (BAQ).
BIS is a self-administered questionnaire consisting of 30 Likert-type items scored from 1 (rarely/never) to 4 (almost always/always) that evaluates overall impulsiveness. It contains several subscales that score attentional impulsiveness (attention and cognitive i n s t a b i l i t y ) , m o t o r i m p u l s i v e n e s s ( m o t o r a n d perseverance) and lack of planning (self-control and cognitive complexity).
The BAQ is a self-administered questionnaire derived from the Aggression Questionnaire developed by Buss and Perry in 1992. It consists of 12 Likert-type items scored from 1 (extremely uncharacteristic of me) to 7 (extremely characteristic of me). The BAQ evaluates overall aggression as a sum of four categories: physical aggression, verbal aggression, anger and hostility.
The Hamilton Depression Rating Scale (HAMD-17) and the Clinical Global Impression Severity Scale (CGIs) were used to confirm the presence of a depressive episode and to evaluate its severity.
The data was analyzed using SPSS 16.0 and Microsoft Office Excel. As the tested variables were ordinal, non-parametric tests were performed.
RESULTS
The group studied was comprised of 103 male patients, with ages between 18 and 80 years old (mean age 45). The age distribution was 13% (n=14) 18-29 years old, 43% (n=44) 30-49 years old, 41% (n=42) 50-69 years old and 3% (n=3) 70+ years old. Three quarters of the patients (n=77) resided in urban areas and 25% of them (n=26) resided in rural areas.
More than half (55%, n=57) were either married or living with a stable partner, 21% (n=22) were never married, 19% (n=19) were divorced and 5% (n=5) were widowed. A small fraction of the patients (18%, n=19) were living alone, the rest living with family or friends (82%, n=84).
Most of the patients (61%, n=63) had a high school level education, 18% of them (n=18) had a lower level education and the rest (21%, n=22) had a higher level education. A large number of patients (43%, n=44) were either on pensions or disability, 29% (n=30) had a stable employment, 11% (n=11) had an unstable employment and 17% (n=18) were unemployed.
Regarding the intensity of the present depressive episode, in most cases it was severe, either with or without psychotic symptoms (53%, n=55 and 26%, n=27 respectively). A small number of patients (19%, n=19) had a medium intensity depressive episode and a minority (2%, n=2) had a low intensity depressive episode. This distribution reflects the fact that, generally only the more severe depressive episodes require hospitalization.
The patients (n=103) were divided into two groups according to the type of hospitalization (voluntary or involuntary).
Fig. 1. Distribution of the types of admission in the studied sample. 56 patients were voluntarily hospitalized, while 47 were hospitalized on a involuntary basis.
1.Tolerance to frustration
The patients with involuntary admission had a significantly lower tolerance to frustration than the ones with voluntary admission (Mann-Whitney U=881.5, n1=47, n2=56, p=0.003), with more patients having a very low tolerance to frustration in the involuntary admission group (fig.2-4).
2.Impulsivity
The impulsivity scores of the involuntarily admitted patients were higher than those of the patients with voluntary admission (Mann-Whitney U=805.5, n1=47, n2=56, p<0.001) , with more patients in the involuntary admittance group having high scores on the BIS. (fig. 5-7)
3.Aggression
There was a marginal statistical difference between the aggressiveness scores in favour of the patients with involuntary admission (Mann-Whitney U = 1 0 4 2 , n 1 = 4 7 , n 2 = 5 6 , p = 0 . 0 5 9 ) ( f i g . 8 – 1 0 ) .
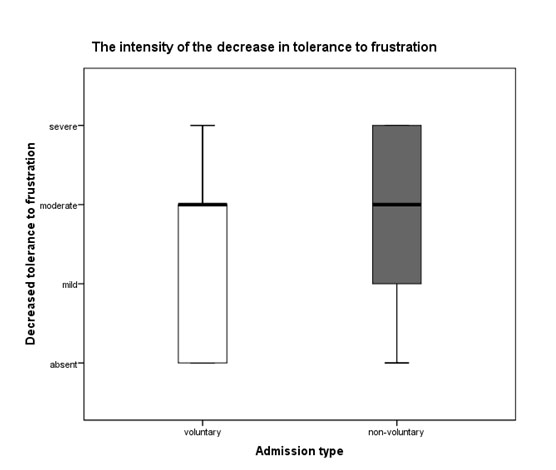
Fig. 2. Boxplots of the distribution of the low tolerance to frustration scores in the (n1=47) and voluntary (n2=56) admittance groups (p=0.003).
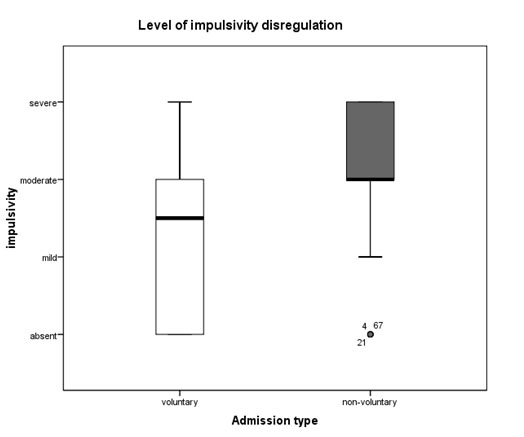
Fig. 5. Boxplots of the distribution of the impulsivity scores in the involuntary (n1=47) and voluntary(n2=56) admittance groups (p<0.001)
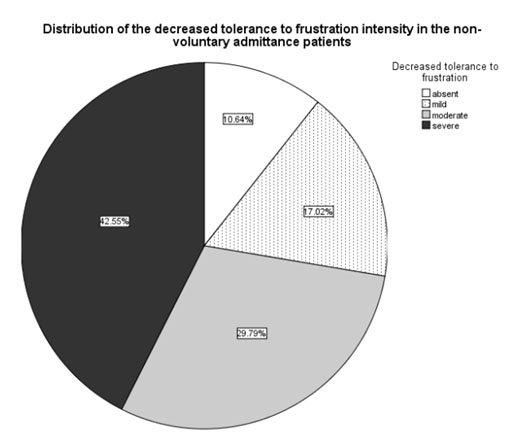
Fig. 3. Prevalence of specific low tolerance to frustration scores in the patients with involuntary (n1=47) admission
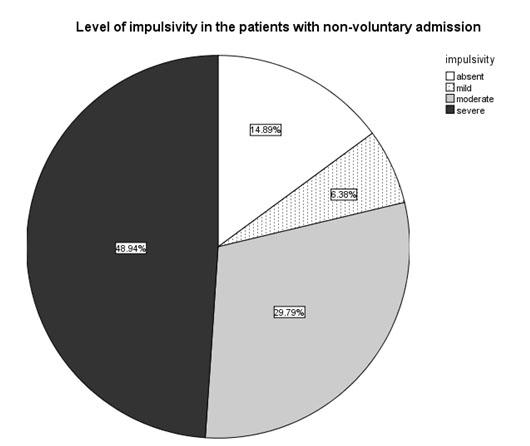
Fig. 6. Prevalence of specific impulsivity scores in the patients with involuntary (n1=47) admission
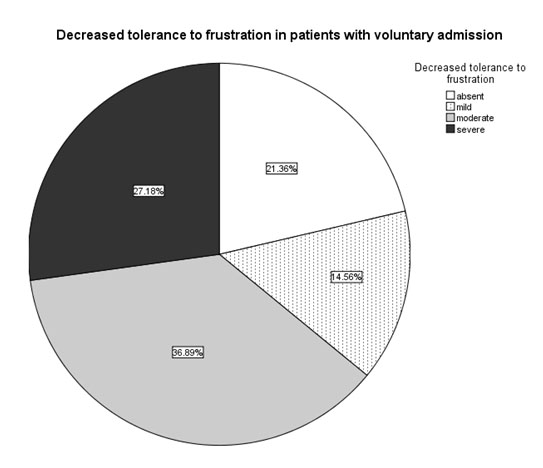
Fig. 4. Prevalence of specific low tolerance to frustration scores in the patients with voluntary (n2=56) admission
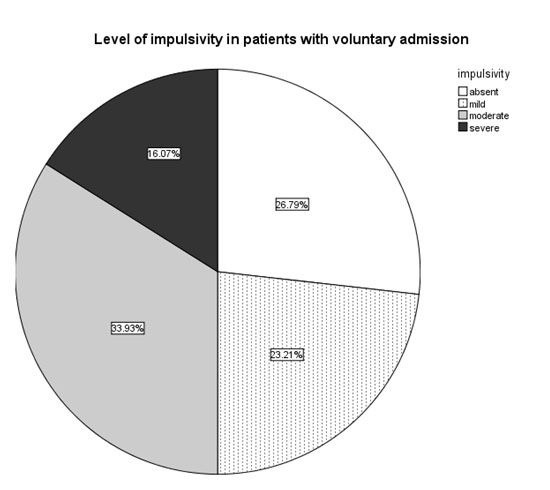
Fig. 7. Prevalence of specific impulsivity scores in the patients with voluntary (n2=56) admission
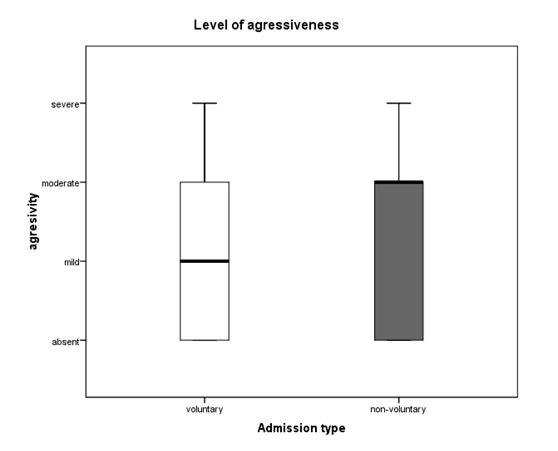
Fig. 8. Boxplots of the distribution of the aggressiveness scores in the involuntary (n1=47) and voluntary (n2=56) admittance groups (p=0.059)
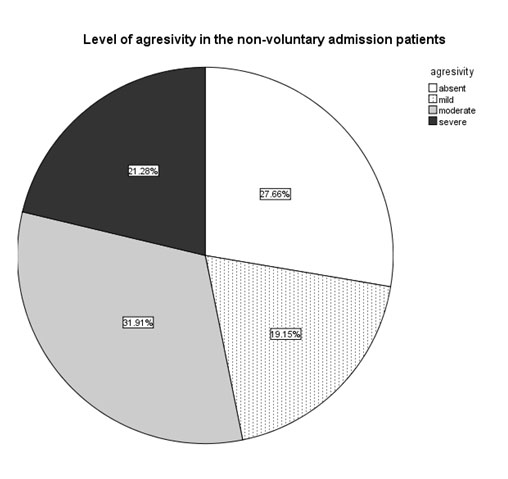
Fig. 9. Prevalence of specific aggressiveness scores in the patients with involuntary (n1=47) admission
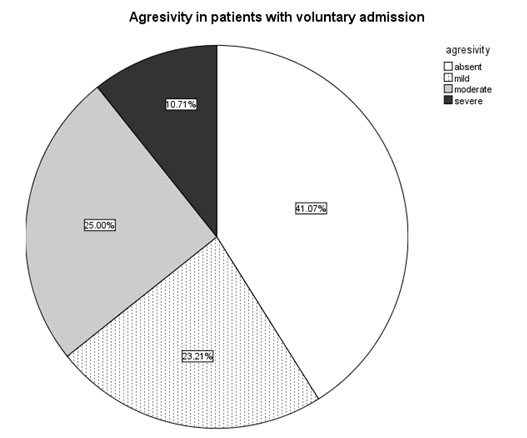
Fig. 10. Prevalence of specific aggressiveness scores in the patients with voluntary (n2=56) admission
4.Irritability
There were no significant differences between the two groups regarding the irritability scores (n1=47, n2=56, Mann-Whitney U=1160, p=0.266).
The irritability scores were strongly correlated with the aggressiveness ones (Spearman’s correlation coefficient= 0.727, p<0.001) , as well as with the impulsivity scores (Spearman’s correlation coefficient= 0.671, p<0.001)(table 1).
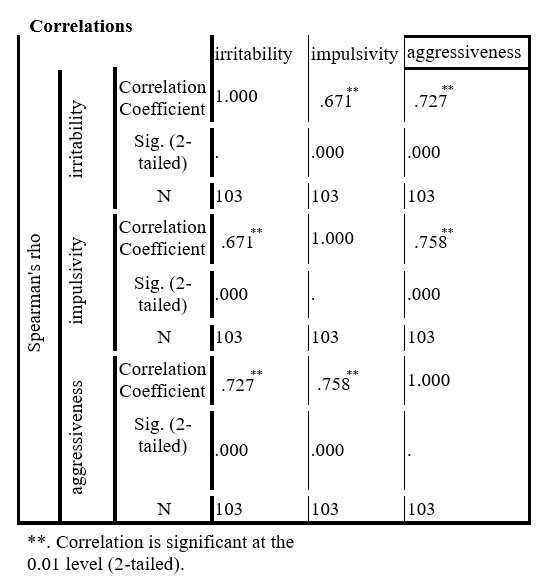
Table 1. The correlations between the scores on the irritability, impulsivity and aggressiveness scales
5.Personality disorders
There were no differences in incidence of voluntary or non-voluntary hospitalization when taking into account each type of personality disorder (Chi- square=4.806, p=0.187, n=103) (table 2). But personality disorder comorbidity (taken as a whole) was more frequent in patients that were hospitalized involuntarily than in those with voluntary hospitalization (53.19% vs 32.14%) (Mann-Whitney U=1035, n1=47, n2=56, p=0.035) – fig. 11 and fig. 12.
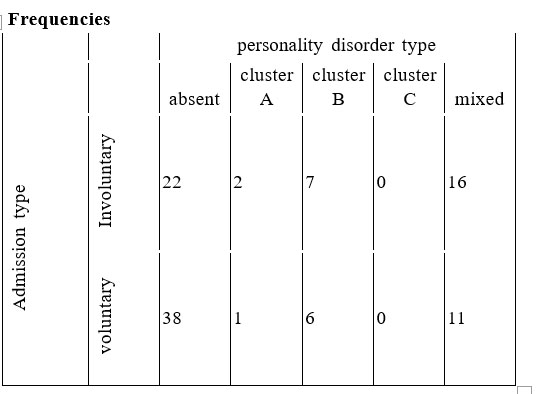
Table 2. Number of patients with voluntary/involuntary admission distributed according to the personality disorders
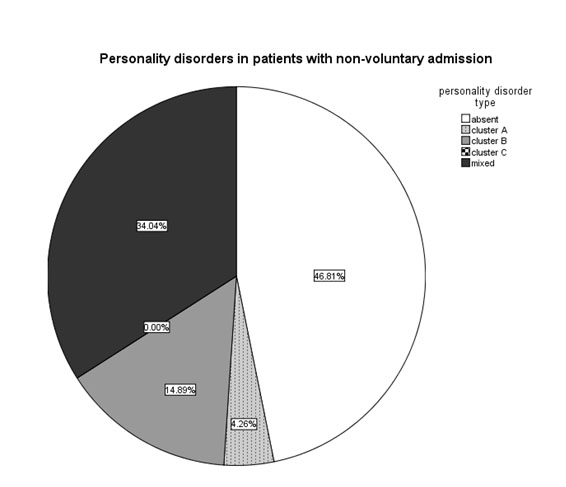
Fig. 11. Personality disorders in patients with involuntary admission (n=47).
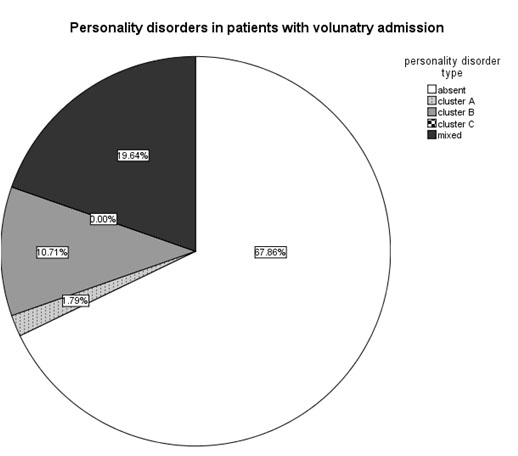
Fig. 12. Prevalence of personality disorders in patients with voluntary admission (n2=56)
DISCUSSIONS
Apart from the behavioural correlation stressed by Mann et al., depression and impulsivity seem to be also linked on a molecular level. Serotonin regulation abnormalities have been tied to both irritability and depressed mood (5, 6, 7). The same neurotransmitter has b e e n i m p l i c a t e d i n t h e m e d i a t i o n o f o t h e r psychopathological traits like aggression and anxiety (5, 6, 7).
In a study on patients with major affective disorders, Oquendo et al slightly modified the diathesis model created by Mann et al. (3), stating that persons who go on to commit suicidal acts after a depressive episode tend to develop more pessimism in response to a stressor and/or have aggressive/impulsive traits (8).
In a review of empirical studies, published in 2001, it was found that impulsivity and aggression were traits consistently associated with completed suicide (9). In another study that compared serious and non-serious suicide attempters, it was found that in the first group there were significantly higher impulsivity, violence, anger-in and anger-out scores (10). Perroud et al., in 2011, studied a sample of patients with major affective disorders. It was found that impulsive and aggressive traits strongly correlated in suicide attempters, independent of diagnosis, but impulsivity distinguished suicide attempters from non-attempters only in the major depressive disorder group, and not in the bipolar disorder group (11). In a psychological autopsy study of 351 suicides, McGirr et al found that impulsivity was a valid risk factor for suicide (12). There are many other studies that found impulsivity and aggression as valid suicide risk factors (13, 14, 15, 16, 17). One review found that the information available regarding anger, irritability and hostility as suicide risk factors is insufficient and more research is needed (18).
A paper published by Oquendo et al in 2000 found that in bipolar suicide attempters compared with bipolar non-attempters there was more lifetime aggression but not more lifetime impulsivity (19). One review, published in 2013, found that impulsivity is not a predictor for repeated suicide attempts (20). Other studies found a correlation between irritability (21, 22, 23, 24, 25, 26, 27, 28) and aggression (29, 30), but not both, and suicide risk.
Our data also found that impulsivity and aggressivity were correlated with suicide risk (p<0.001, p=0.059 respectively).
Another strong correlation found in our sample was between aggression/impulsivity and the irritability present during the present depressive episode (p<0.001 in both cases), but there was no significant correlation between irritability and suicide risk (p=0.266). In the literature we found few studies that addressed the issue of irritability as a suicide risk factor (31, 32, 33, 34, 35, 36). The results of these studies are in contradiction: three of them found a correlation (32, 33, 34) while the other three found no statistical significance regarding irritability as a suicide risk factor (31, 35, 36). This is an area that requires further research.
T h e h i g h c o r r e l a t i o n b e t w e e n t r a i t aggression/impulsivity and irritability is an interesting find suggesting that a subtype of patients might present with a predominantly irritable clinical aspect of the depressive episode. This is of particular importance in the diagnosis of a depressive episode, since irritability is not included as a symptom either in the DSM IV-TR criteria or in most scales that evaluate depression. It would be easy to misdiagnose such a patient. As a consequence, the patient’s suicide risk might be evaluated as being lower that it actually is.
In our sample we also found a strong correlation between a low tolerance to frustration and suicide risk (p=0.003). This is an area where virtually no research exists. Generally, this variable has been associated with personality disorders. While it is true that in our sample patients with comorbid personality disorders were more frequent in the suicide risk group, the high correlation between a low tolerance to frustration and suicide risk was not fully explained by the existence of this comorbidity.
LIMITATIONS
This study was conducted on male inpatients. Further research is needed in order to determine whether these results can be extrapolated to the general population.
CONCLUSIONS
The data obtained from our study confirms the importance of evaluating trait impulsivity and trait aggression while evaluating suicide risk in depressive male patients. The degree of irritability was not correlated with suicide risk in our sample, but this is an area that has had little research and a definite conclusion cannot be drawn as yet. A possible new suicide risk factor was identified as being low tolerance to frustration. Further research is needed in this area.
REFERENCES
1.World Health Organization. Preventing suicide a global imperative 2014. Available from: http://www.who.int/mental_health/suicide- prevention/world_report_2014/en/
2.Harris EC, Barraclough B. Suicide as an outcome for mental disorders. A meta-analysis. Arch Gen Psychiatr 2005;62(6): 617-27.
3.Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry
1999;156(2): 181-9.
4.Appleby L, Dennehy JA, Thomas CS et al. Aftercare and clinical characteristics of people with mental illness who commit suicide: a case- control study. Lancet 1999;353(9162): 1397-400.
5.Gonda X, Rihmer Z, Zsombok T et al. The 5HTTLPR polymorphism of the serotonin transporter gene is associated with affective temperaments as measured by TEMPS-A. Affect Disord 2006;91(2-3): 125-31.
6.Young SN, Leyton M. The role of serotonin in human mood and social interaction. Insight from altered tryptophan levels. Pharmacol Biochem Behav 2002;71(4): 857-65.
7.Carver CS, Johnson SL, Joormann J. Two-Mode Models of Self- Regulation as a Tool for Conceptualizing Effects of the Serotonin System in Normal Behavior and Diverse Disorders. Curr Dir Psychol Sci 2009;18(4): 195-199.
8.Oquendo MA, Galfalvy H, Russo S et al. Prospective study of clinical predictors of suicidal acts after a major depressive episode in patients with major depressive disorder or bipolar disorder. Am J Psychiatry 2004;161(8): 1433-41.
9.Conner KR, Duberstein PR, Conwell Y et al. Psychological vulnerability to completed suicide: a review of empirical studies. Suicide Life Threat Behav 2001;31(4): 367-85.
10.Gvion Y, Horresh N, Levi-Belz Y et al. Aggression-impulsivity, mental pain, and communication difficulties in medically serious and medically non-serious suicide attempters. Compr Psychiatry 2014;55(1): 40-50.
11.Perroud N, Baud P, Mouthon D et al. Impulsivity, aggression and suicidal behavior in unipolar and bipolar disorders. J Affect Disord 2011;134(1-3): 112-8.
12.McGirr A, Séguin M, Renaud J et al. Gender and risk factors for suicide: evidence for heterogeneity in predisposing mechanisms in a psychological autopsy study. J Clin Psychiatry 2006;67(10): 1612-7.
13.Pompili M, Innamorati M, Raja M et al. Suicide risk in depression and b i p o l a r d i s o r d e r : D o i m p u l s i v e n e s s – a g g r e s s i v e n e s s a n d pharmacotherapy predict suicidal intent? Neuropsychiatr Dis Treat 2008;4(1): 247-55.
14.Dumais A, Lesage AD, Alda M et al. Risk factors for suicide completion in major depression: a case-control study of impulsive and aggressive behaviors in men. Am J Psychiatry 2005;162(11): 2116-24.
15.Apter A, van Praag HM, Plutchik R et al. Interrelationships among anxiety, aggression, impulsivity, and mood: a serotonergically linked cluster? Psychiatry Res 1990;32(2): 191-9.
16.Wang L, He CZ, Yu YM et al. Associations between impulsivity, aggression, and suicide in Chinese college students. BMC Public Health 2014;14: 551.
17.Michaelis BH, Goldberg JF, Davis GP et al. Dimensions of impulsivity and aggression associated with suicide attempts among bipolar patients: a preliminary study. Suicide Life Treath Behav
2004;34(2): 172-6.
18.Brezo J, Praris J, Turecki G. Personality traits as correlates of suicidal ideation, suicide attempts, and suicide completions: a systematic review. Acta Psychiatr Scand 2006;113(3): 180-206.
19.Oquendo MA, Waternaux C, Brodsky B et al. Suicidal behavior in bipolar mood disorder: clinical characteristics of attempters and nonattempters. J Affect Disord 2000;59(2): 107-17.
20.Beghi M, Rosenbaum JF, Cerri C, Cornaggia CM. Risk factors for fatal and nonfatal repetition of suicide attempts: a literature review. Neuropsychiatr Dis Treat 2013;9: 1725-36.
21.Cáceda R, Durand D, Cortes E et al. Impulsive choice and psychological pain in acutely suicidal depressed patients. Psychosom Med 2014;76(6): 445-51.
22.Dvorak RD, Lamis DA, Malone PS. Alcohol use, depressive symptoms, and impulsivity as risk factors for suicide proneness among college students. J Affect Disord 2013;149(1-3): 326-34.
23.Boisseau CL, Yen S, Markowitz JC et al. Individuals with single versus multiple suicide attempts over 10 years of prospective follow-up. Compr Psychiatry 2013;54(3): 238-42.
24.Links P, Nisenbaum R, Ambreen M et al. Prospective study of risk factors for increased suicide ideation and behavior following recent discharge. Gen Hosp Psychiatry 2012;34(1): 88-97.
25.Neufeld E, O’Rourke N. Impulsivity and hopelessness as predictors of suicide-related ideation among older adults. Can J Psychiatry
2009;54(10): 684-92.
26.Sublette EM, Carballo JJ, Moreno C et al. Substance use disorders and suicide attempts in bipolar subtypes. J Psychiatr Res 2009;43(3): 230-8.
27.Carballo JJ, Akamnonu CP, Oquendo MA. Neurobiology of suicidal behavior. An integration of biological and clinical findings. Arch Suicide Res 2008;12(2): 93-110.
28.Swann AC, Dougherty DM, Pazzaglia PJ et al. Increased impulsivity associated with severity of suicide attempt history in patients with bipolar disorder. Am J Psychiatry 2005;162(9): 1680-7.
29.Mousavi SG, Keramatian K, Maracy MR, Fouladi M. Suicidal ideation, depression, and aggression among students of three universities of isfahan, iran in 2008. Iran J Psychiatry Behav Sci 2012;6(1): 47-53.
30.Baca-García E, Oquendo MA, Saiz-Ruiz J et al. A pilot study on differences in aggression in New York City and Madrid, Spain, and their possible impact on suicidal behavior. J Clin Psychiatry 2006;67(3): 375- 80.
31.Judd LL, Schettler PJ, Corvell W, Akiskal HS, Fiedorowicz JG. Overt irritability/anger in unipolar major depressive episodes: past and current characteristics and implications for long-term course. JAMA Psychiatry 2013;70(11): 1171-80.
32.Perlis RH, Fraguas R, Fava M et al. Prevalence and clinical correlates of irritability in major depressive disorder: a preliminary report from the Sequenced Treatment Alternatives to Relieve Depression study. J Clinical Psychiatry 2005;66(2): 159-66.
33.Perlis RH, Fava M, Trivedi MH et al. Irritability is associated with anxiety and greater severity, but not bipolar spectrum features, in major depressive disorder. Acta Psychiatr Scand 2009;119(4): 282-9.
34.Pompili M, Innamorati M, Giupponi G et al. Predicting risk of suicide in bipolar and unipolar depression: correlation between temperament and personality. Nervenarzt 2009;80(3): 315-23.
35.Wolfersdorf M, Kiefer A. Depression and aggression. A control group study on the aggression hypothesis in depressive disorders based on the Buss-Durkee Questionnaire. Psychiatr Prax 1998;25(5): 240-5.
36.Pawlak J, Dmitrzak-Węglarz M, Skibińska Mr et al. Suicide attempts and clinical risk factors in patients with bipolar and unipolar affective disorders. Gen Hosp Psychiatry 2013;35(4): 427-32.
***



