Cognitive and emotional correlates of posttraumatic stress symptoms in train drivers exposed to work trauma
Abstract
Introducere.O serie de cercetări internaţionale au evidenţiat riscul ocupaţional al mecanicilor de locomotivă de a fi expuşi la incidente feroviare cu potenţial traumatic şi de a dezvolta simptome de stres posttraumatic şi alte tulburări comorbide.Deşi frecvenţa incidentelor ,,persoană sub tren” este crescută, puţini dintre mecanicii de locomotivă expuşi la acestea, raportează ulterior simptome de stres posttraumatic. Obiective. Scopul studiului actual este de a identifica ce anume îi diferenţiază pe mecanicii cu simptome de stres posttraumatic cauzate de implicarea în incidentele traumatice şi de a explora diferenţele individuale ca factori de risc pentru dezvoltarea ulterioară a simptomelor postraumatice. Metode. 129 de mecanici de locomotivă expuşi la incidente PST au completat un chestionar demografic, Scala Revizuită a Impactului Evenimentelor, Indexul Stării g e n e r a l e d e s ă n ă t a t e , I n v e n t a r u l c o g n i ţ i i l o r posttraumatice şi Inventarul distresului peritraumatic. Rezultate.Analiza statistică a datelor a evidenţiat diferenţe importante privind cogniţiile posttraumatice şi impactul emoţional peritraumatic al incidentelor PST între mecanicii de locomotivă cu simptome de stres posttraumatic şi cei ce nu raportează ulterior simptome. În particular, am identificat că relaţia dintre distresul peritraumatic şi simptomele de stres traumatic este mediată parţial de auto-blamare. Concluzii. Rezultatele obţinute evidenţiază necesitatea de a include factorii de risc cognitivi şi emoţionali în programele de prevenţie şi intervenţie specifice pentru mecanicii de locomotivă implicaţi în incidentele PST
INTRODUCTION
Post traumatic stress disorder (PTSD) represents the most investigated form of a posttraumatic reaction. According to the DSM IV TR (2000), the current standard for diagnosing mental disorders, PTSD is characterized by three distinct types of symptoms including re- experiencing of the event, avoidance patterns and persistent hyperarousal(1). Although epidemiological studies highlight that most people are confronted at least once in their lifetime with events of traumatic intensity, prevalence of posttraumatic stress disorder in the general population is relatively low (2).
Thus, traumatic exposure is neccesary, but not enough for developing PTSD. In consequence, researchers have directed their efforts to identifing the most influential risk factors that predict specific symptom development (3,4). Meta-analytic studies emphasized the relevance of distinct risk factors classified as pretraumatic, peritraumatic and posttraumatic. Conclusions (3,4) highlight the importance of traumatic event particularities, as well as individual characteristics that may put the person at risk of being traumatised. In light of recent findings, instead of dealing with isolated risk factors, there is a need to see how these factors interact influencing the person’s reaction to trauma and the experience of subsequent symptoms.Thus, trauma researchers’ current recomandations strongly suggest the need to identify risk pathways or mechanisms, underlying their relationship to outcome variables (5). Diversity of identified risk factors and different trajectories of vulnerability are proof of the fact that one cannot evaluate trauma reaction outside of the specific context of confrontation.
Person-under-train (PUT) accidents are serious rail incidents, resulting in violent death or injury of persons, because of accidentally or intentionally falling in front of the moving train (6). They consist of railway suicides, accidents or collisions of vehicles with the locomotive at level crossings. Being frequently exposed to these work incidents, train drivers are susceptible of developing posttraumatic reactions, and researchers have tried to identify risk factors that raise train drivers’ vulnerability to trauma.
Most studies investigate circumstantial factors that may influence train drivers’s response to trauma, like frequent exposure to job related incidents or severity of their consequences (7,8). Studies support the need to investigate the role of individual differences in the development and maintenance of PTSD symptoms in train drivers involved in PUT incidents(9,10).
Current perspective on the development and persistence of PTSD symptoms emphasizes the role of cognitive appraisal of the traumatic experience as a fundamental mediator in the posttraumatic adaptation process (11). Cognitive models of PTSD (12-14) assert that dealing with trauma produces alterations in the generic cognitive schemas about the world, self and others. Exposed persons’ perspective and belief system is being affected by the traumatic event, so that the world is perceived to be unsafe and threatening, and the self is seen as lacking the resources and skills needed to cope with the adversive environment (14,15).
Presence of these negative beliefs about oneself and the world, as a result of a traumatic encounter, represents the essential vulnerability factor for specific PTSD symptoms. Catastrophic interpretation that these central negative beliefs generate, involves retrospective exaggeration of traumatic events, and/or the permanent appraisal of being at risk to be exposed to a new trauma(14).
Cognitive distortions about the world and the self proved to be strong predictors of PTSD diagnosis, as they can discriminate between all trauma exposed individuals, those that developed clinically significant symptoms (16,17). Studies in samples with various types of trauma provide strong empirical support for the relationship between the altered beliefs about the self and the world and the frequency and severity of posttraumatic symptoms (16-19). Also, challenging and modifing these beliefs in cognitive-behavioral therapy for traumatised people has been effective in reducing specific symptoms PTSD (20).
In terms of work related trauma confrontation one study found that posttraumatic stress was predicted by pretrauma catastrophic thinking in a sample of firefighters exposed to on the job traumatic incidents (21). This risk factor may be essential for train drivers as well, because, although most of them are confronted with at least one PUT incident during their years of duty, studies show that just a few develop persistent PTSD symptoms (9). According to a french study(7), the traumatic potential of these incidents is mainly determined by the fact that the train driver may feel responsible for the death of the victims.
Another relevant risk factor for the development and persistence of PTSD symptoms, is peritraumatic emotional reactivity. A meta-analysis of risk factors for PTSD (4), highlighted that compared with pretraumatic factors (like previous traumatic history, family psychopathology, etc.), peritraumatic response was a stronger predictor (intensity of emotional reactivity during trauma, life threat perception during adversive event, peritraumatic dissociation).
Context of traumatic encounter does not imply life threat for the train driver and also dissociation is less likely to occur in these specific confrontations. In stead, differences in peritraumatic emotional intensity may be of relevance for the susbsequent development of PTSD symptoms in these proffesionals, as a particularity of trauma related to accidents. Studies provide empirical support for the relationship between increased intensity of emotional reaction during traumatic confrontation with motor vehicle accidents, disasters and subsequent PTSD symptoms (22-26).
An interesting and complex risk path or mechanism combines these two factors: the appraisal of the traumatic event and the peri-traumatic emotional reaction to it. Interpretation of the event may influence the subsequent development of the peri-traumatic reaction, which further on, will lead to the reinterpretation of the event and of the peritraumatic reaction to it (5). This chained reaction to PUT incidents may influence train drivers’ subsequent distress levels, and we consider further investigating it.
2.OBJECTIVES:
The present study aims to investigate differences in appraisal and emotional reactivity to PUT incidents between train drivers that report PTSD symptoms and those who do not report being affected by these incidents . Also, we want to investigate the way that cognitive interpretation and emotional reaction to PUT incidents combine in predicting subsequent distress in exposed train drivers.
Specific objective 1: To investigate differences between train drivers who report severe symptoms of PTSD and those without symptoms, in terms of the investigated risk factors. H 1a: We expect to identify a significantly higher level of negative posttraumatic cognitions for train drivers that report symptoms of PTSD as opposed to train drivers (without PTSD symptoms). H 1b: Also, we expect that the intensity of peritraumatic distress will be significantly more frequently reported as higher by train drivers that report PTSD symptoms as opossed to the symptom free train drivers.
Specific Objective 2: To investigate the relationship between risk factors (posttraumatic cognitions, intensity of peritraumatic distress) and reported level of PTSD symptoms. H 2a: We expect to find a positive significant relationship between risk factors (posttraumatic cognitions, peritraumatic distress intensity) and high levels of PTSD symptoms. H 2b: Also, we hypothesize that posttraumatic cognitions mediate the relationship between intensity of peritraumatic emotional reaction to PUT incidents and subsequent PTSD symptoms.
3. MATERIALS AND METHODS:
3.1.Procedure
As a first step we obtained the approval for research objectives and procedure from the Head of the Railway Regional Department of Cluj, that allowed us access to train drivers involved in Traffic Safety. Selection of participants was done on a voluntary basis. Of the 176 initially approached train drivers, 12 refused to participate, and 35 declared they never had an PUT incident. Questionnaires and an informed consent were completed individually, during three proffesional training meetings.
3.2.Participants
129 drivers (mean age = 37.8, SD= 8.19) belonging to locomotive depots in Cluj, Dej, Bistrita and Brasov were included in the final sample. The average frequency of PUT incidents throughout train driver’s career was 3.43 (SD= 2.86).
3.3.Instruments
3.3.1. Impact of Events Scale-Revised -IES-R (27) has been used extensively to identify the specific symptoms of PTSD in relation to a specific traumatic event. The questionnaire contains 22 items, has adequate psychometric qualities and it is used to assess the three categories of posttraumatic symptoms: reexperiencing the traumatic event, avoidance and hypervigilance, according to diagnostic criteria for PTSD in DSM IV. Also, the questionnaire has adequate power to discriminate between people with severe symptoms of PTSD and less affected persons (28). In our sample, internal consistency was appropriate(=0.89).
3.3.2. Index of general health –GHQ-28 (29). GHQ-28 is commonly used as a screening tool, highlighting the increased risk for certain mental disorders: severe depression, symptoms of anxiety and sleep disorders, somatic disorders, social difficulties (isolation from others).Internal consistency for the present s a m p l e w a s a d e c q u a t e ( = 0 . 7 1 ) .
3.3.3. Posttraumatic cognitions inventory (PTCI) was developed by Foa, et al.(1999) to assess cognitive distortions that dealing with trauma may produce. With excellent psychometric qualities, the instrument is a measure commonly used in research of posttraumatic pathology. Subscales of negative cognitions about the self and the world prove relevant predictors of the onset and maintenance of PTSD symptoms (17-19,
21). Also, the questionnaire adequately discriminates individuals who meet diagnostic criteria for PTSD (16). For the present sample, internal consistency was appropriate ( 0.82).
3.3.4. Peritraumatic distress inventory-PDI (30) is a useful tool in investigating emotional reactivity to trauma. The instrument has adequate psychometric qualities and is an effective method for assessing the diagnostic criterion A2 for PTSD. According to factorial analysis conducted by the authors, the instrument measures two independent factors: intensity of emotional reactivity and perception of life being threatened during the traumatic event. Internal consistency for the study is appropriate ( 0.77).
3.3.5. Demographic questionnaire regarding personal information (age, tenure, marital status, etc.), number of PUT incidents, details of the most significant incident.
4. RESULTS :
4.1. Evaluation of differences between train drivers that reported PTSD symptoms and those without symptoms
Testing the first hypothesis required dividing the sample into three categories.The first category consisted of those who reported no psychological distress as a consequence of PUT experiences. 13 participants were included in this category, reporting complete absence of PTSD symptoms, although they were exposed to PUT incidents. Also the number of general psychological symptoms, assessed using the GHQ-28 questionnaire is significantly reduced in this category when compared to the other train drivers (t = 3.48, p = 0.02).
We followed current reccomendations (28) and used the cut-off value of 33 (of max. 88, on the global IES- R scale) to differentiate train drivers who report clinically significant PTSD symptoms. 16 of the participants had scores above 33, corresponding to a of clinical level of PTSD symptoms’ intensity.
The third group (N = 100) consisted of the majority of train drivers involved in the study, who reported some specific PTSD symptoms, because of the PUT incidents, but their scores were low when compared to the cut-off value used in screeening for PTSD.
To assess differences between the three groups in terms of the risk factors investigated, we performed a series of analyses of variance ANOVA one-way for each of the evaluated factors. Table 1 summarizes the descriptive data for the three categories of participants and the significance of differences between them.
According to performed ANOVA analysis, the three categories of train drivers-without PTSD symptoms, with few PTSD symptoms and with clinically relevant PTSD symptoms, reported statistically significant differences in beliefs about self, the world, the level of self-blame and the intensity of peritraumatic distress. As hypothesized, train drivers without symptoms of PTSD had significantly lower average levels of negative cognitions when compared to the category of train drivers with more severe and frequent PTSD symptoms. Results comparing means of the two groups are depicted in Table 2, for each type of cognition separately, for the global cognition scale, as for the peritraumatic distress intensity.
Differences between groups confirm that, unlike train drivers that did not report symptoms of PTSD, more affected train drivers make negative interpretations of self and world and also make internal attributions of r e s p o n s i b i l i t y f o r t h e i n c i d e n t s . In terms of reported peritraumatic emotional reaction, the average reactivity reported by train drivers in the group without PTSD symptoms (m = 11.61, S.D. = 1.12) was significantly lower than that of the group with symptoms of PTSD (m = 15.06, S.D. = 3.21). Greater peritraumatic intensity of distress was reported by train drivers that also report more frequent PTSD symptoms (t = – 3.67, df = 27, p = 0.00).
4.2. Assessment of the relationship between risk factors a n d r e p o r t e d P T S D s y m p t o m s In assessing risk factors for the development of
PTSD symptoms for train drivers involved in PUT incidents, we identified significant associations between variables that discriminated between train drivers that report symptoms of PTSD and those who are not affected by such events. These factors are summarized in Table 3.
In line with findings from other studies, current findings support the positive association of posttraumatic cognitions about the self (r = 0.45, p = 0.01) and the world (r = 0.27, p = 0.01) and reported PTSD symptoms. The more negative the individual views the self and the world, the higher the level of posttraumatic symptoms he reports. When considering effect size of significant correlations, the relationship between negative cognitions about the self and the frequency of PTSD symptoms has the strongest pragmatical impact (r² = 0,20) among the three types of posttraumatic cognitions. Perception of self as incompetent, or lacking ability to cope with trauma may be a relevant predictor of persistence of PTSD symptoms for train drivers involved in PUT incidents.
Also self-blaming cognitions were significantly positively associated with PTSD symptoms (r = 0.38, p = 0.01). The determination coefficient for this relationship also demonstrates a strong effect size (r²= 0,14). If the train driver considers himself blameworthy for causing the incident, the level of PTSD symptoms he reports will be greater. Relationship with this risk factor is particularly relevant because the context of PUT incidents leaves room for negative interpretation on the adequacy of their behavioral reaction in the situation and may cause the train driver to hold himself responsible for the accident.
Peritraumatic distress intensity was also significantly positively correlated with the presence of posttraumatic stress symptoms (r = 0.41, p = 0.01), with a strong effect size (r² = 0, 16). If the intensity of peritraumatic emotional distress was reported to be high, subsequent reported levels of PTSD symptoms were also higher.
Results confirm our expectations regarding relevant cognitive and emotional correlates of PTSD symptoms for train drivers involved in PUT incidents.
4.3. Mediation analysis
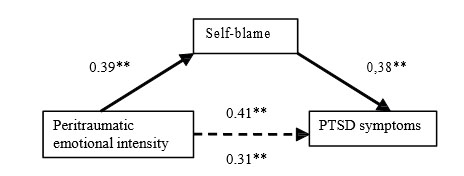
According to current criteria for mediation analysis (31), we checked if posttraumatic cognitions satisfy necessary conditions as mediator of the relationship between emotional peritraumatic reaction and PTSD symptoms. The predictor needs to be associated with both the mediator and the outcome variable and, after controlling for the effects of the mediator, the relation between predictor and outcome should reduce partially or completely, accounting for partial mediation or total mediation. Results showed that preconditions were satisfied only for self-blame as the mediator variable, because this was the only posttraumatic cognition that significantly correlated to both outcome (PTSD symptoms) and predictor (peritraumatic emotional intensity). The diagram below shows results of the mediational analysis we performed.
The recommended methodology (31) uses hierarchical regression analysis to assess if the relationship between peritraumatic emotional reaction(predictor) and PTSD symptoms(outcome variable) modifies when controlling for self-blame(mediator). All regression beta coefficients were significant. Adding self-blame to the equation significantly decreased the amount of variance in PTSD symptoms explained by peritraumatic emotional intensity. The Sobel test(32) used to test the indirect effect for this mediation was found to be significant, 1,80 (p <0.03). According to results, self-blame acts as a significant partial mediator on the relationship between peritraumatic emotional intensity and PTSD symptoms.
5. DISCUSSION AND CONCLUSIONS:
Results revealed important issues on each of the investigated risk factors and their interaction in predicting PTSD symptoms.
5.1. Negative cognitions about the self, world, and self- blame
Results of the present study confirm the hypothesis derived from cognitive models of PTSD, for train drivers exposed to trauma. It is interesting that in the current study, negative cognitions about self, world, and self-blame are factors that significantly differentiate train drivers with clinical symptoms of posttraumatic stress from those that did not exhibit such symptoms. These results are consistent with contemporary models of PTSD development (13, 14). According to Ehlers & Clark’s cognitive model of PTSD persistence, posttraumatic symptoms are prevalent when appraising trauma experiences causes a sense of serious current threat and the perception that the individual does not have the ability to surpass the consequences of extreme stressors.
In particular, negative cognitions about the self and self-blame were found to be important correlates of PTSD symptoms and differentiating factors between train drivers that manage to adapt efficiently after PUT experiences and those who report significant posttraumatic distress. It is possible that exposure to PUT incidents may determine train drivers to perceive they lack necessary resources to cope with these reccurent traumatic events, which, according to theoretical and empirically supported perspectives, predicts persistent symptoms of PTSD. Results are congruent with other studies that involved on the job risk for trauma. For example, negative beliefs about oneself was found to be a relevant prospective predictor for the development and maintenance of posttraumatic symptoms in firefighters (21).
Particularly for train drivers exposed to PUT incidents, internal atribution of responsibility or feeling guilty after the traumatic encounter, seems to be associated with later posttraumatic distress. Because they are the agents that drive the locomotive, train drivers have a higher probability to consider themselves blameworthy for the accidents and responsible for fatalities. It is important to note that most of the time the train cannot be stopped because of high speed, and other technical limits, so collision is often unavoidable. Interpreting their reaction to the PUT incident as inadequate or insufficient may elicit changes in the way train drivers perceive themselves and the world, which in turn, leads to an impaired posttraumatic adaptation process and the appearance of PTSD symptoms. This particularity is congruent with anterior research on train drivers, highlighting the need to offer information about trauma and posttraumatic symptoms and construct behavioral protocols for these specific contexts (7).
Present findings on negative cognitions developed by train drivers, also have a pragmatic impact. Negative trauma-related cognitions can be processed in daily life and in therapy by offering new, incompatible information (33). Working through negative cognitions about the self and especially self-blame, may be an efficient way to minimize the traumatic impact of recurrent PUT incidents in train drivers and subsequent PTSD symptoms.
5.2. Intensity of peritraumatic distress
Another relevant correlate for the persistence of PTSD symptoms we found, was the magnitude of distress retrospectively reported by the train driver during the PUT incident. Investigation of this risk factor involves both an emotional intensity generated by being involved in a traumatic event (PUT incident) and psychophysiological reactivity indices. We found that peritraumatic distress intensity is significantly lower for train drivers that didn’t report symptoms of PTSD, and a significant correlate of PTSD symptom levels. However, this result must be interpreted keeping in mind that present data are retrospective self-reports and that we couldn’t control the effects of inaccurate memory over time.
Still, results regarding the relevance of this particular risk factor are congruent to other anterior studies, on survivors of motor vehicle accidents (26) or survivors of different types of disasters (34).
A surprising result was the significant association of peritraumatic distress with self-blame. The more train drivers reported feeling responsible for the incidents, the stronger was the intensity of their peritraumatic reaction. Using mediation analysis, we tested for a chained reaction between peritraumatic intensity of distress, negative posttraumatic cognitions and PTSD symptoms.We found self-blame to partially mediate the relationship of peritraumatic distress and PTSD symptoms. This result is congruent with current research in PTSD risk factors in stressing that synergistic response to trauma is determined as a cumulative action of variables.
5.3. Concluding remarks
In interpreting the results we should consider some limitations of the current research. First, cross- sectional design that we used makes it impossible to draw any conclusions about causality. This is a first study that highlights significant relationships between cognitive and emotional correlates of trauma and PTSD symptoms in train drivers involved in PUT incidents. It would be therefore beneficial to evaluate the relationship between predictor variables and PTSD symptoms in a longitudinal design.
Second, we exclusively used retrospective self-report data, a common feature in trauma research. This data collection method does not allow precise determination of the specific timing of symptom development and the way they correlate with exposure to traumatic PUT incidents. In addition, given that the assessment was done at unequal intervals of time since the traumatic event, it is possible that the results are influenced by the responders’ memory accuracy. We tried to control the effect of other factors in determining traumatic symptoms, by asking participants to report psychological distress exclusively caused by PUT experiences. But we need to consider the possibility that the results were influenced by other variables that were not assessed: history of previous trauma, negative current life events, influence of protective factors as well, that should be considered in further research.
Also, conclusions about the reported differences between categories of train drivers with and without PTSD symptoms are dependent on the method of determining the categories. The procedure used was recommended in previous studies that reported adequate sensitivity and specificity of IES-R for the cut-off value we used (28).
However, establishing a cut-off value is somewhat arbitrary and taxometric studies have reccomended a dimensional structure for PTSD as opposed to a categoric one (35).
Although it is a first study regarding the relations between studies variables, our results contribute to understanding the development of posttraumatic stress symptoms for train drivers exposed to trauma in their professional environment. Findings support the need for replication studies. Also, they highlight the need to include individual risk factors, in particular posttraumatic cognitions and peritraumatic distress, as relevant to prevention and intervention programs tailored for train drivers exposed to PUT incidents.
Abreviation list
PTSD: Postraumatic stress disorder
PUT incidents: ,,person-under-train” incidents
IES-R: Impact of Event Scale-Revised GHQ-28: General Health Questionnaire PTCI : Posttraumatic Cognitions Inventory PDI: Peritraumatic Distress Inventory
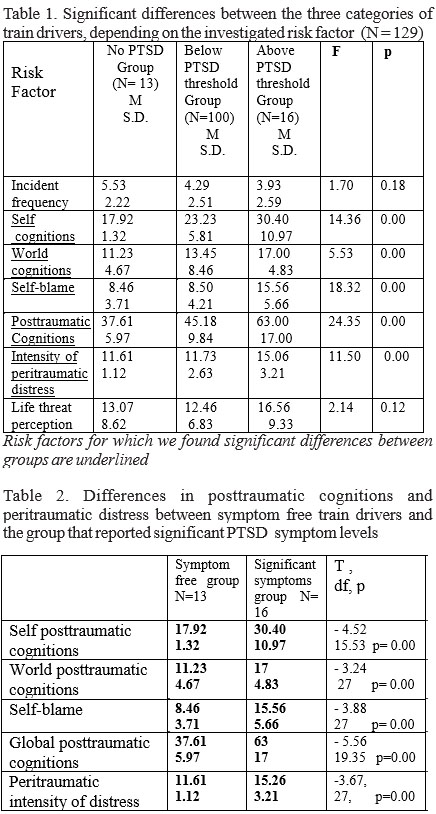
Table 3 Intercorrelations between risk factors and PTSD symptoms (N=129)
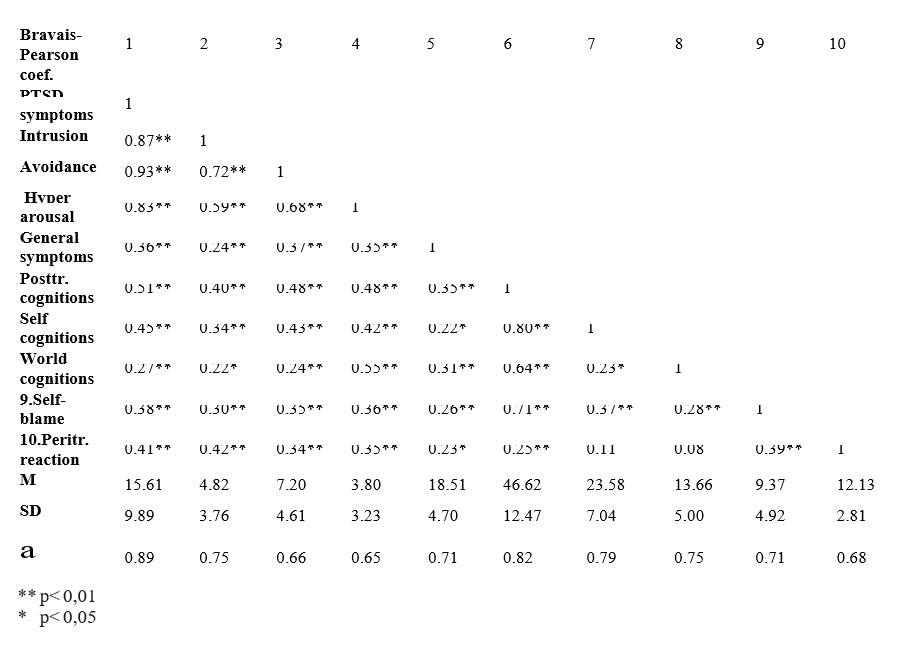
Fig. 1. Mediation diagram for peritraumatic emotional intensity as predictor of PTSD symptoms with self-blame as mediator
References :
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (revised 4th ed). Washington (DC): American Psychiatric Association, 2000
2. Litz, B. T., Gray, M. J., Bryant, R., Adler, A. B. Early intervention for trauma: Current status and future directions. Clin Psychol: Sci Pr 2002; 9: 112-134.
3. Brewin, C.R., Andrews, B., Valentine J.D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000; 68: 748–766.
4. Ozer, E. J., Best, S. R., Lipsey, T. L., Weiss, D. S. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychol Bull 2003; 129: 52–73.
5. Kallay, E. Trauma. From pathology to growth, ASCRED, Cluj- Napoca , 2011
6.Theorell T., Leymann H., Jodko M., Konarski K., Norbeck H.E., Eneroth P. „Person under train” incidents: medical consequences for subway drivers. Psychosom Med 1992 ;54(4): 480-488
7.Cothereau C., De Beaurepaire C., Payan C., Cambou J.P., Rouillon F., Conso F. Professional and medical outcomes for French train drivers after „person under train”accidents: three year follow up study. Occup Environ Med 2004; 61(6): 488 – 494
8. Siol T., Schaefer A., Thomas W., Köhle K. Posttraumatic Stress Symptoms in Train Drivers Following Serious Accidents: A Pilot Study. European Psychotherapy 2003;4(1): 3-9
9. Lunt, J., Hartley, R. Literature Review of Post Traumatic Stress D i s o r d e r a m o n g s t R a i l W o r k e r s 2 0 0 4 ; www.hse.gov.uk/research7hsl_pdf/2004/hsl0416.pdf
10. Yum B.S., Roh J.H., Ryu J.C., et al. Symptoms of PTSD according to individual and work environment characteristics of Korean railroad drivers with experience of person-under-train accidents. J Psychosom Res 2006; 5: 691-717
11. Dunmore, E.C., Clark, D.M., & Ehlers, A. A prospective investigation of the role of cognitive factors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. Behav Res Ther 2001; 39: 1063-1084.
12.Foa, E. B., Rothbaum, B. O. Treating the trauma of rape: Cognitive behavioral therapy for PTSD. New York: Guilford Press, 1998
13.Ehlers A, Clark DM. A cognitive model of posttraumatic stress disorder. Behav Res Ther 2000; 38:319–415.
14.Dalgleish, T. Cognitive approaches to posttraumatic stress disorder (PTSD): The evolution of multi-representational theorizing. Psychol Bull, 2004; 130: 228–260
15. Foa EB, Cahill SP Psychological therapies: Emotional processing. In Smelser, NJ Bates PB (eds), International Encyclopedia of Social and Behavioral Sciences, Oxford, UK, Elsevier, 2001
16. Foa EB, Ehlers A, Clark DM, Tolin DF, Orsillo SM . The Posttraumatic Cognitions Inventory (PTCI): development and validation. Psychol Assessment 1999; 11:303–314
17. Beck, J.G., Coffey, S.F., Palyo, S.A., Gudmundsdottir B., Miller, L.M., Colder, C.R. Psychometric Properties of the Posttraumatic Cognitions Inventory (PTCI): A Replication With Motor Vehicle Accident Survivors, Psychol Assessment 2004; 16(3), 289–298.
18. Cieslak, R., Benight, C.C., Lehman, V. Coping Self-Efficacy Mediates the Effects of Negative Cognitions on Posttraumatic Distress, Behav Res Ther 2008; 46: 788-798
19. Startup, M., Makgekgenene, L., Webster, R. The role of self-blame for trauma as assessed by the Posttraumatic Cognitions Inventory (PTCI): a self-protective cognition?, Behav Res Ther 2007; 45(2):395- 403.
20. Foa EB, Rauch SAM. Cognitive changes during prolonged exposure versus prolonged exposure and cognitive restructuring in female assault survivors with PTSD. J Consult Clin Psychol 2004; 72:879–884.
21.Bryant R.A., Guthrie, R.M. Maladaptive appraisals as a risk factor for posttraumatic stress: a study of trainee firefighters, Psych Sci 2005;
16(10):749-52
22.Bernat, J.A., Ronfeldt, H.M., Calhoun, K.S., Arias, I. Prevalence of traumatic events and peritraumatic predictors of posttraumatic stress symptoms in a nonclinical sample of college students, J Traum Stress 1998; 11:645–665
23.Brewin CR, Andrews B, Rose, S. Fear, helplessness, and horror in posttraumatic stress disorder: investigating DSM-IV criterion A2 in victims of violent crime. J Traum Stress, 2000; 13:499–509
24. Simeon, D., Greenberg, J., Knutelska, M., Schmeidler, J., Hollander, E. Peritraumatic Reactions Associated With the World Trade Center Disaster. Am J Psych 2003; 160:1702-1705
25. Birmes, P., J., Brunet, A., Coppin-Calmes, D. Symptoms of Peritraumatic and Acute Traumatic Stress Among Victims of an I n d u s t r i a l D i s a s t e r , P s y c h S e r v 2 0 0 5 ; 5 6 ( 1 ) : http://ps.psychiatryonline.org
26. Daisuke, N.,Yutaka, M., Naohiro, Y., Hiroko, N.,Yoshiharu, K., Shigenobu, K. Peritraumatic Distress Inventory as a predictor of post- traumatic stress disorder after a severe motor vehicle accident, Psychiatry Clin Neurosci, 2010 ; 64(2): 149-156.
27.Weiss, D.S., Marmar, C.R. The Impact of Event Scale—Revised. In Wilson JP, Keane TM.(eds.). Assessing Psychological Trauma and PTSD: A Practitioner’s Handbook. New York, Guilford, 1997: 399–411
28.Creamer, M., Bell R., Failla S. Psychometric properties of the Impact of Event Scale—Revised , Behav Res Ther 2003; 41(12) : 1489-1496
29.Goldberg DP , Hillier VF. A Scaled Version of the General Health Questionnaire. Psychol Med 1979; 9: 139-145
30.Brunet, A., Weiss, D.S., Metzler, T.J. et al. The Peritraumatic Distress Inventory:A Proposed Measure of PTSD Criterion A2. Am J Psychiatry 2001; 158:1480–1485
31. Baron, R.M., Kenny, D.A. The moderator-mediator variable distinction in social psychology research: Conceptual, strategic and statistical considerations. J Pers Soc Psychol 1986; 51: 1173-1182
32. Preacher, K.J., Leonardelli, G.J.Calculation for the Sobel test : An i n t e r a c t i v e c a l c u l a t i o n t o o l f o r m e d i a t i o n a l t e s t s 2 0 0 1 ; http://people.ku.edu/preacher/sobel/sobel.htm
33. Hagenaars, M.A., van Minnen, A., Rooij, M. Cognitions in prolonged exposure therapy for posttraumatic stress disorder. Int J Clin Health Psychol 2010; 10(3):421-434
34. Grimm, A., Hulse, M., Preiss, L. , Schmidt, S. Post- and peritraumatic stress in disaster survivors: an explorative study about the influence of individual and event characteristics across different types of disasters. Eur J Psychotraumatol 2012; 3: 10.3402/ejpt.v3i0.7382
35. Ruscio, A. M., Ruscio, J., & Keane, T. M.. The latent structure of posttraumatic stress disorder: A taxometric investigation of reactions to extreme stress. J Abnorm Psychol 2002; 111(2): 290-301.
***



