METHADONE MAINTENANCE TREATMENT AND SEXUAL FUNCTION OF HEROIN ADDICTED PATIENTS
Abstract
A significant number of patients treated for heroin addiction suffer from sexual disorders. The aim of this research was to investigate the sexual function of the heroin addicted patients taking a methadone maintenance treatment (MMT), to identify the types of sexual disorders and analyse their causes. Methods: Questionnaire, scale ASEX and WHO-ASSIST V3.0 were performed by 20 sexually active patients (15 men and 5 women), undergoing MMT. Results: The data of the questionnaire have shown that 55% of the patients suffer from deterioration of their sexual function, 30% of the patients have observed the improvement of their sexual function, and 15% of the patients have not felt any changes. The patients with a worsened sexual status have taken higher daily dosage of methadone (66, 8 ± 24,11 mg). 40% of the patients have expressed the anxiety caused by the disturbance of their normal sexual function, it being known that the duration of their treatment was longer and the dosage of methadone was higher (p ˃ 0,05). According to ASEX scale, the men scored 14,13 ± 2,85 Likert points, and the women - 15,6 ± 2,88 Likert points; 5 patients (25%) have not had any sexual disorders, 4 patients(70%) have observed some disorders of their sexual functioning, and only one patient (5%) has suffered from sexual dysfunction. In general, a fade of the sexual desire (3, 25 ± 1,06 Likert points) and problems with achieving orgasm (3,0 ± 0,85 Likert points) were noticed, but the experienced orgasm was satisfactory (2,6 ± 0,99 Likert points). The patients showing relatively good indicators for the libido (2.5 Likert points), the arousal (2.3 Likert points), the satisfaction with orgasm (2,0 Likert points) took 40-50 mg of methadone per day. A marked decrease of the sexual desire, the disturbance of the ejaculatory function (3.5 Likert points), the dissatisfaction with orgasm were noted at the dosage of 80- 100 mg of methadone per day. Conclusions: The methadone has an effect on the sexual function. High doses suppress the sexual desire, delay the ejaculation and prevent the achievement of orgasm, the average doses do not lead to obvious sexual disorders caused by the abuse of heroin.
Introduction
At present the sexual dysfunction is a widespread phenomenon among the general population: about 43% of women and 31% of men suffer from sexual disorders of different severity. (1).
According to the medical statistics, there were 11259 patients with drug addiction in the Republic of Moldova in
2016, and 3721 of them are injecting drug users (2). In 2002, the first pilot-project of substitution treatment with buprenorphine of the heroin-dependent patients was launched in the Republic of Moldova. Since 2004, the programme of methadone substitution therapy (MST) has been running in Moldova. By today (31.12.2016), 1662 addicted patients have received methadone.
Heroin addiction is not only a social, legal, economic, political problem, but also a sexual one. The patients taking part in MMT programme often complain of decrease of the sexual desire and the lack of a sexual life. This is undoubtedly related to the disruptive effect of the heroin on the hypothalamic-pituitary-gonadal axis, leading to an imbalance in the endocrine system (3): men suffer from an erectile dysfunction, women – from menstrual irregularities. Therefore, heroin addicts often resort to amphetamine-type stimulants to maintain the elements of their sexuality. We have noticed that the desire to improve family relationship is a frequent motivation for applying for the MMT treatment programme.
By its origin, the methadone is a synthetic opioid agonist to the opioid receptors and it has similar pharmacological effects with heroin (4), but differs from it in the duration of action. Methadone is a long-acting opioid (5) with the duration of action of 24-36 hours (6,7,8), while heroin (diacetylmorphine) is a short-acting opioid, the duration of its action is 6 hours (9,10).
Materials and methods
The research involved 20 patients (15 men and 5 women) suffering from heroin addiction and ongoing a methadone maintenance therapy (MMT) in the drug treatment clinic. They voluntarily accepted to participate in the study. 20 people completed the study, so no one was eliminated, no one left the programme. The inclusion criteria were: heroin addicted patients who have been under MMT for at least 2 months, the existence of a temporary or a permanent sexual partner at the time of the research.
The questionnaire included two main parts: the objective data and the subjective experiences. The objective data contain information about the age, the duration of MMT, the dose of methadone. The subjective experiences include the changes in the sexual status before and after the MMT (better / worse / no change), the attitude towards the current sexual function (worried / not worried).
The clinical sexology study was conducted by means of the ASEX-scale (Arizona Sexual Experience Scale) – a special questionnaire which allows to obtain detailed information about the status of the sexual sphere. The questionnaire includes five questions, each estimated from 1 to 6 points by the Likert scale. In total, it is possible to get from 5 to 30 points, the more points the patient gets, the more pronounced sexual dysfunctions he has. The
number of points ≥ 21 for women and ≥ 20 for men
c o r r e s p o n d s t o a c l i n i c a l l y d e t e c t a b l e s e x u a l dysfunction;15-20 points for women and 11-19 points for men indicate the boundary disorder of the sexual function;
≤ 14 points for women and ≤ 10 points for men mean the
absence of a sexual dysfunction. At the same time the sexual dysfunction scale was used for the comparative evaluation of the patients taking different doses of methadone. The problems connected with the consumption of alcohol, tobacco and drugs were detected by ASSIST V3.0 (The Alcohol, Smoking and Substance Involvement Screening Test), which is a short questionnaire for the screening of the psychoactive substances abuse. We used it to identify the abuse of psychoactive substances during the treatment with methadone. The statistical analysis was performed using the statistical calculator Microsoft Windows version 6.1and the software Student Test (test t-Student). The threshold of the statistical significance is the value p<0.05. No comorbidities were diagnosed. At the same time, at the beginning of the treatment, the patients were requested to warn the researchers, if other medication was administered.
The results
On the basis of the data obtained by means of WHO- ASSIST V3.0 scale, we have concluded that 19 patients (95%) completely have given up using heroin, seven patients (35%) still abuse alcohol, 2 people (10%) use marijuana, 3 people (15 %) – cocaine and 1 person (5%) – amphetamine. All patients are heavy smokers.
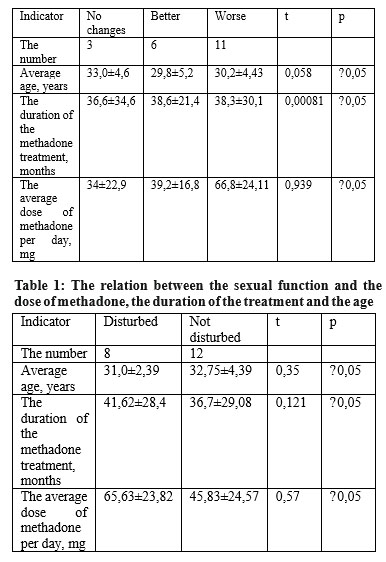
As Table 1 shows, against the background of the methadone maintenance treatment, the number of patients suffering from the deterioration of their sexual function is higher than the number of those ones whose sexual functions have improved (p ˃ 0,05). The duration of MMT is longer and the daily dose of methadone is higher in the group of the patients whose sexual functions worsened (p
˃ 0,05).There is no significant age difference between the two groups (p ˃ 0,05).
Over the half of the patients (60%) have not expressed any worries about their present sexual functioning, in their case the daily dose of methadone (p ˃ 0,05) is lower than the dosage of those patients who have expressed concerns. At the same time, the patients who are worried about the sexual function take the methadone treatment of longer duration (on average- 5 months or longer) (p ˃ 0,05).
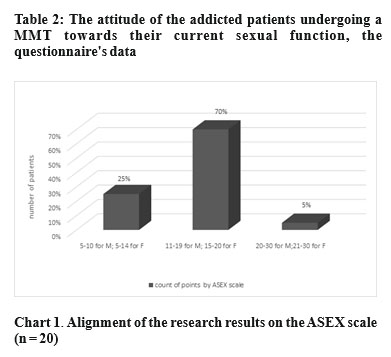
The score by the ASEX scale was 14,13 ± 2,85 for men and 15,6 ± 2,88 for women (t = 0,36, p ˃ 0,05), although men complained of sexual weakness, but women did not express such complaints at the time of the interview. Perhaps, it can be explained by gender differences: women tend to satisfy their partner, hiding their sexual lethargy, while men shun or reject the partner, fearing the failure (11). According to the ASEX scale, 5 patients (25%) have not expressed any signs of the sexual dysfunction, 14 patients (70%) have observed some disorders of the sexual functioning, and only one man (5%) has suffered from sexual dysfunction. (Chart 1).
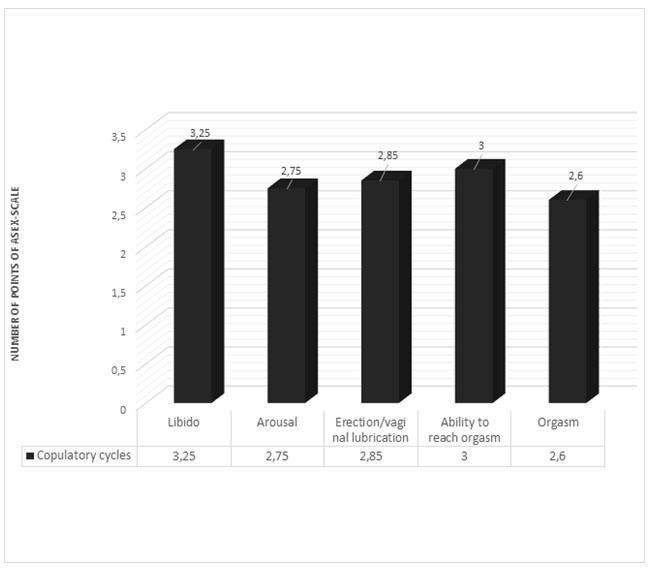
As Chart 2 shows, the sexually active patients taking MMT have observed the failing of the sexual desire (3,25 ± 1,06 points Likert) and problems with achieving orgasm (3,0 ± 0,85 points Likert). Despite it, their orgasm satisfied them (2,6 ± 0,99 points Likert). It should be noted that, in response to a question about the sexual desire, the patients also complained of the lack of appetite and initiative. The lack of the desire or of the motivation to do something dominated the patient’s mind, and the problem of libido was not strongly pronounced against this background.
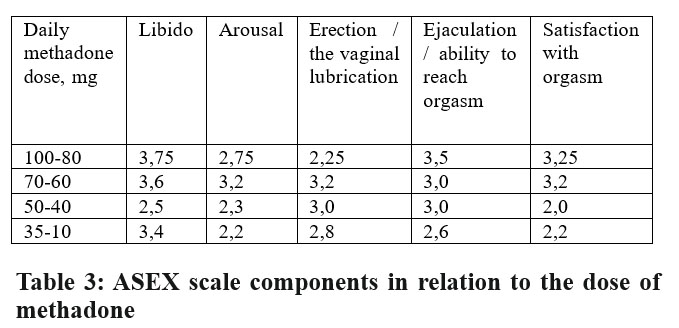
The patients showing relatively good indicators for the libido (2.5 points Likert), the arousal (2.3 points Likert), the satisfaction with orgasm (2.0 points Likert) took 40-50 mg of methadone per day (Chart 3). A marked decrease of the sexual desire (3.75 points Likert), the ejaculatory function disorders (3.5 points Likert), the dissatisfaction with the orgasm (3.25 points Likert) were noted at a dose of 80-100 mg of methadone per day (Chart
3). Table 3 shows that increasing doses of methadone exacerbate the severity of the ejaculatory and orgasmic disorders.
Discussion
The unhindered sexuality plays an important role in the quality of life and this is also true for the patients with psychiatric illnesses (12). The individual complex therapeutic strategy for the patients with opioid dependence should be directed to improving the quality of life (13). The medication-based strategy of treating the opiate dependence by the administration of methadone causes sexual dysfunction in many cases (12). Most clinicians avoid asking the patients questions of a sexual nature (14). Discussing the sexual dysfunction induced by medication is crucial for the patients’ adherence to the treatment (12), as the presence of a sexual dysfunction may provoke a risk of returning to heroin abuse (11,14). The spectrum of the sexual dysfunctions in the patients receiving MMT is mainly represented by the erectile dysfunction, the fade of the libido and the inability to achieve the orgasm. Some research also describe the disorders of all the aspects of the sexual activity – a global dysfunction (15,16,17,18). The recent data predominantly point out the suppression of the libido (libido inhibition)
and the reduced sexual pleasure (decreased sexual pleasure) (11). Neurophysiologists speak about different levels of disorders: central – the limbic system where the sexual desire or the libido is formed, and peripheral – the spinal cord where there are spinal erection centres that ensure the mechanical aspect of the intercourse. Erectile dysfunction is highly prevalent among men abusing opioids (19,20) but the level of testosterone is not low in all cases.(16). Some researchers explain it by the hypogonadism and the depression (17,18). The androgenic treatment of such patients is not very effective (21). The erectile dysfunction significantly depends on the duration of the Methadone therapy and the Methadone daily dosage (18). On the other hand, a number of studies show no correlation between the duration of the methadone treatment and sexual disorders (22), but a dependence of the latter on the dose of the drug (15,22). So, a lot of criticism against MMT and conflicting data can be found in the specialised medical literature.
Conclusions:
Methadone has an effect on the sexual function. High doses suppress the sexual desire, delay the ejaculation and prevent the achievement of orgasm. The average doses do not cause such changes.
During the treatment with methadone, the problems related to the sexual dysfunction, caused by the abuse of heroin, get smoothed: the discontinuation of heroin consumption enables the recovery of the sexual function, and the methadone helps the patient to improve the quality of life, eliminating the painful withdrawal phenomena.
References:
1.Delgado P.L., Brannan S.K., Craig H. et al. Sexual functioning assessed in 4 double-blind placebo- and paroxetine-controlled trials of duloxetine for major depressive disorder // J Clin Psychiatry. 2005 Jun; 66(6):686-92
2.Indicatori preliminari în format prescurtat privind sănătatea populaţiei şi activitatea instituţiilor medico-sanitare pe anii 2015-2016. Centrul Național de Management în Sănătate. Chișinău, 2017; pag.179. www.cnms.md.
3.Trajanovska AS, Vujovic V, Ignjatova L, Janicevic-Ivanovska D, Cibisev A. Sexual dysfunction as a side effect of hyperprolactinemia in methadone maintenance therapy // Med Arh. 2013; 67(1):48-50.
4.LI Hong, YANG Liang, YANG Huiying, et al. The changes of hypothalamic pituitary gonadal function in heroin addiction // J Chinese Medical Journal, 1995, 75(7):421-422.
5.Charles E. Argoff, MD and Daniel I. Silvershein, MD. A Comparison of Long- and Short-Acting Opioids for the Treatment of Chronic Noncancer Pain: Tailoring Therapy to Meet Patient Needs // Mayo Clin Proc. 2009 July; 84(7): 602–612.
6.Fridman L., Flemihg N., Roberts D., Hyman S. Sourse book of substanve abuse and addiction. Williams and Wilkins, 2000, p.194
7.Иванец Н.Н.. Лекции по наркологии.Издание второ е, переработанное и расширенное. М.: «Нолидж»,2000. — 448 с.. 2000
8.Wolff, K. & Hay, A.W.M. (1994) Plasma methadone monitoring with methadone maintenance treatment. Drug & Alcohol Dependence, 36, 69-71
9.Kim Wolff, Sarah Welch & John Strang. Specific laboratory investigations for assessments and management of drug problems // Advances in Psychiatric Treatment 1999, vol. 5, pp. 180-191
10.Gyr E, Brenneisen R, Bourquin D, Lehmann T, Vonlanthen D, Hug I. Pharmacodynamics and pharmacokinetics of intravenously, orally and rectally administered diacetylmorphine in opioid dependents, a two- patient pilot study within a heroin-assisted treatment program // Int J Clin Pharmacol Ther. 2000 Oct; 38(10):486-91.
11.Xia Y, Zhang D, Li X, et al. Sexual dysfunction during methadone maintenance treatment and its influence on patient’s life and treatment: a qualitative study in South China // Psychol Health Med. 2013;18(3):321- 9.
12.Cohen S, Kühn KU, Sträter B, Scherbaum N, Weig W. Adverse side- effect on sexual function caused by psychotropic drugs and psychotropic substances // Nervenarzt. 2010 Sep;81(9):1129-37
13.Ненастьева А.Ю. Качество жизни у больных с зависимостью от опиатов ( Клинико-терапевтические корреляции). Диссертация на соискание ученой степени кандидата медицинских наук. Москва, 2007.
14.Chekuri V, Gerber D, Brodie A, Krishnadas R. Premature ejaculation and other sexual dysfunctions in opiate dependent men receiving methadone substitution treatment // Addict Behav. 2012 Jan;37(1).
15.Brown R., Balousek S., Mundt M., Fleming M. Methadone Maintenance and Male Sexual Dysfunction // Journal of Addictive Diseases, Volume 24, Issue 2, 2005.
16.Cioe P., Friedmann P., Stein M. Erectile Dysfunction in Opioid Users: Lack of Association with Serum Testosterone // Journal of addictive diseases 2010 Octomber; 29(4):455-460
17.Hallinan R, Byrne A, Agho K, McMahon C, Tynan P, Attia J. Erectile dysfunction in men receiving methadone and buprenorphine maintenance treatment. The Journal of Sexual Medicine [2008, 5(3):684-692]
18.Tatari F, Farnia V, Nasiri RF, Najafi F. Trazodone in methandone induced erectile dysfunction // Iran J Psychiatry. 2010 Fall;5(4):164-6.
19.Quaglio G, Lugoboni F, Pattaro C, Melara B; G.I.C.S, Mezzelani P, Des Jarlais DC; G.I.C.S. Erectile dysfunction in male heroin users, receiving methadone and buprenorphine maintenance treatment // Drug Alcohol Depend. 2008 Apr 1;94(1-3):12-8.
20.Babakhanian M, Alam Mehrjerdi Z, Shenaiy Y. Sexual dysfunction in male crystalline heroin dependents before and after MMT: a pilot study // Arch Iran Med. 2012 Dec;15(12):751-5.
21.Buvat J, Lemaire A, Ratajczyk J. Role of hormones in sexual dysfunctions, homosexuality, transsexualism and deviant sexual behavior: diagnostic and therapeutic consequences // Contracept Fertil Sex. 1996 Nov; 24(11):834-46.
22.Zhang Y, Wang P, Ma Z, Xu Z, Li Y. Sexual function of 612 male addicts treated by methadone // Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2011 Aug;36(8):739-43
***


