EFFICIENCY OF INTERVENTION PROGRAMS FOR SEXUAL OFFENDERS
Abstract
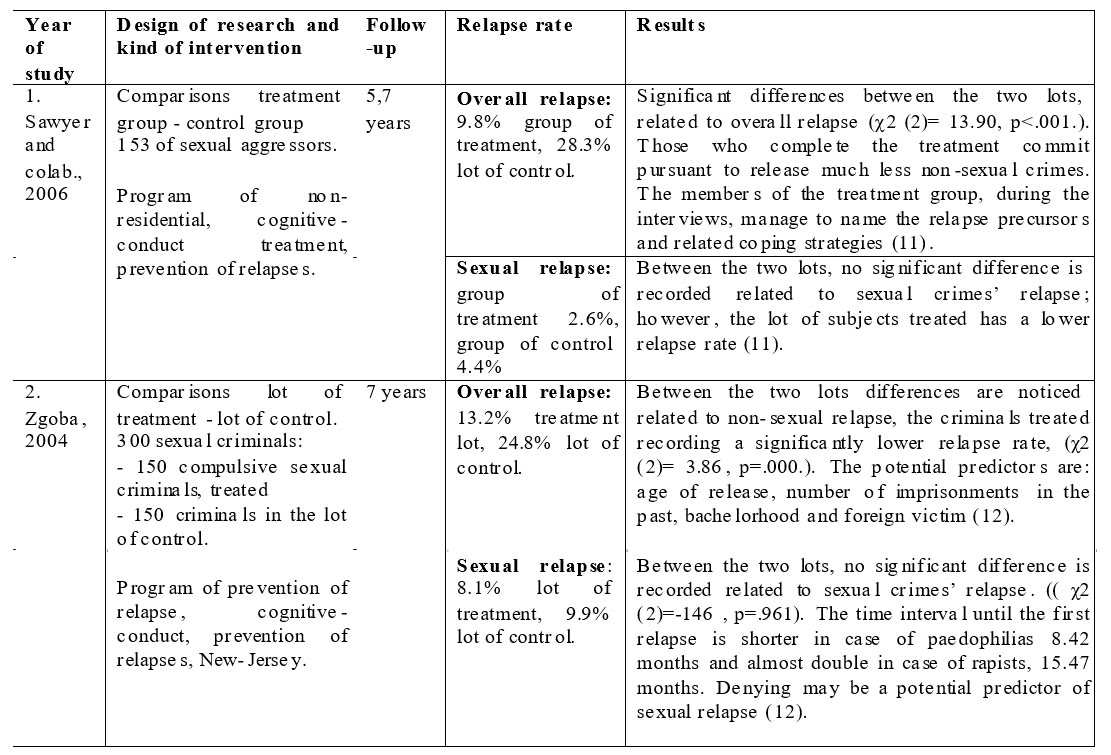
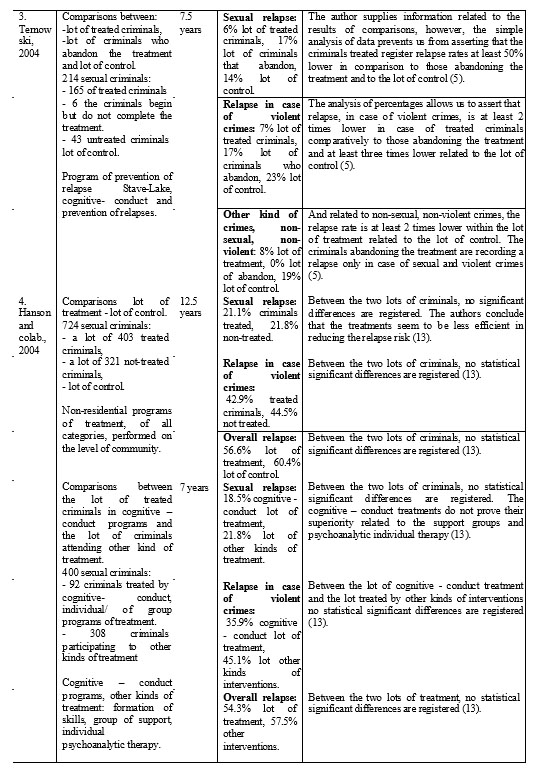
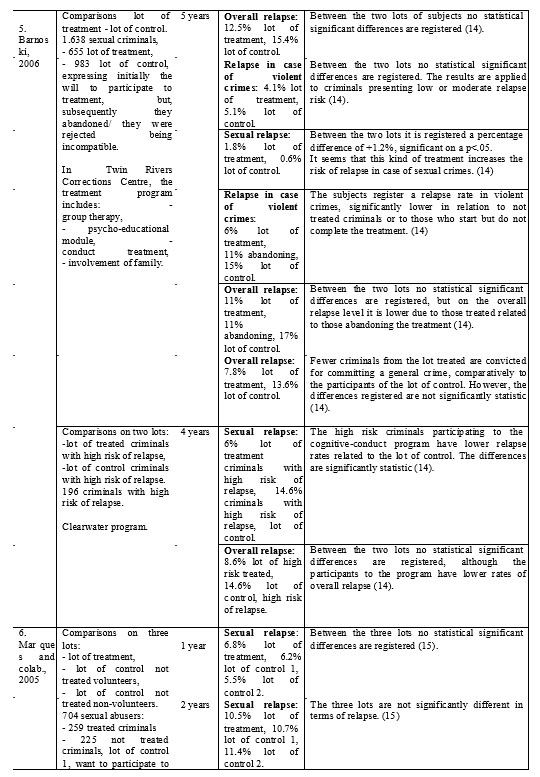
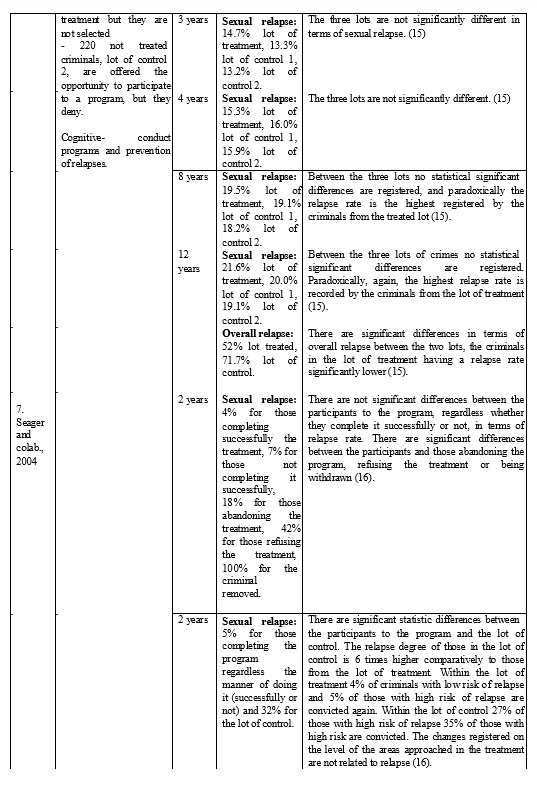
The article presents the factors in relation to which the efficiency of the programs for the reduction of relapse risk in the case of sexual aggressors is determined. Also, there are presented and discussed the advantages and the limits of the kinds of design encountered in the studies which verify the efficiency of the programs. Further on, there are synthesised the results of some researches which compare the experimental lot – controls the lot or makes comparisons between participants, which complete or refuse or abandon the treatment, report the overall relapse rate, specific or in violent crimes for such category of criminals.
Examining the specialised literature related to the efficiency of treatment programs for sexual abusers, a question is raised: which are the factors in terms of which we may assert that an intervention program operates. There are several answers to this question, formulated based on the analysis of the studies published.
Harkins and Beech (2007) perform an extensive presentation of the kinds of design used in the evaluation of treatment efficiency in case of sexual aggressors, and these are: randomised control trial, descriptive design, „risk band” analyses, incidental design, statistic control of differences between groups, groups of comparison adjusted, change in case of treatment and meta-analysis (1).
Thus, the randomized clinical study (RCT) involves that criminals are aleatorily introduced in the group of treatment and control. In this case, the post- treatment differences noticed may be assigned to intervention; any changes appeared during the initial phase, being assigned to hazard. When one turns to quasi- experimental designs, it is difficult to provide a compatible lot of comparison. It is important in determining the compatibility to consider the equivalent risk of a new conviction of the subjects of the two lots.
The RCT approach involves simultaneous observance of the following two conditions: aleatory assignment of volunteers in the group of treatment and control, as well as the integrity of intervention (treatment to be implemented exactly according to the manual). As limits of this kind of design, Marshall & Marshall (2006) enumerates: difficulty of checking the integrity of treatment, necessity of hundreds of criminal populations out of which to be extracted aleatorily the two lots, contamination of the results of non-treated lot of volunteers due to negative emotions which they may express (2). In addition, the „blind” enforcement of manuals affects, according to the authors, „the therapeutic craft” of clinicians and interferes simultaneously to the principle of responsivity. The comparisons to those that abandon the treatment would be unfair, being mainly about motivated and non-motivated criminals. The recommended variables used in the analysis between the two groups are: number of victims, sex of victim, use of violence or a weapon, duration of abuse. Equally important is the fact that, besides static variables, the groups are compatible as well in terms of relevant dynamic variables. Since the role of therapist is essential, representing between 40% and 60% of the benefits of treatment, the authors conclude that it is much limited by strict use of manual. The alternatives proposed are those of incidental design and evaluation based on the comparisons between the relapse rates registered and those expected for the group treated.
The „risk band” analyses compare the relapse rates of a treated group to those anticipated/expected based on some measurements of relapse risk. This kind of design is useful provided that the treatment is available to all criminals, being non-ethical that one turns to forced construction of a lot of control not treated. The advantage of this kind of design consists in the fact that it may be implemented retrospectively.
The incidental design compares a group of treated individuals to a group that, based on objective reasons, did not receive treatment (belongs to other period of time and the names are extracted from archives, these were to be released before the completion of treatment, there was no resource meant to allow that all convicts benefit from treatment). In such cases, it is presumed that the groups of treatment are approximately identical.
Another means is that of statistic control of differences between groups, being compared a lot of treated criminals to another not-treated. If we do not consider the variables related to the risk of criminals, the conclusions may be distorted.
Another alternative is that of matched control groups, corresponding to the lot of treatment on the level of some dimensions related to relapse. Since the dimensions related to risk are multiple, it is possible to be excluded some important variables.
The change within the treatment is another reason why it involves the analysis of the manner in which the participants present modifications on the level of intervention targets. A method is represented by the calculation of clinical significant change or Real Change Index or comparison of successfully treated criminals to those considered unsuccessfully treated. Thus, an individual is evaluated as benefiting from a treatment if there is a significant statistic and clinical change between the pre and post-treatment operation. This kind of demarche is highly conditioned by the quality of (accuracy and validity) measurement instruments, as well as by the desirability of answers supplied by participants.
M e t a – a n a l y s i s i s r e c o m m e n d e d s i n c e , combining quantitatively the results of several studies, it may identify as well a small size of effect due to the numerous pattern reunited. The method raises problems as well: low rate of new convictions for sexual crimes, problems in encountering a relevant lot of control, differences in terms of the duration of follow-up periods, low number of participants to all treatment groups, differences registered on the level of the means of evaluation used by individual programs, low rates of abandoning the programs.
A descriptive design concerns the following of a group of treated criminals and determining the relapse average of it pursuant to the completion of program in the absence of a lot of control. This approach related to the impact of treatment over the group on the whole, ignores the differences related to the style of teaching of subjects, of motivation, skills and their psycho-social operation. Another important limit of this kind of design concerns the fact that it may not be determined whether the differences noticed are due to hazard or other possible factors.
Perkins and colab. (1998) state that, when we refer to the evaluation of a treatment the following factors should be considered:
-integrity of treatment – extent to which the treatment was provided as conceived to be applied,
-impact of treatment – degree of effect and impact of the treatment over the issues where it interferes based on its pattern,
-results of treatment – the extent to which the treatment improves on long term „the surviving rates” (reduced relapse) by reporting to the criminals not included in such treatment (3).
The impact studies of treatment present the effects thereof on a number of parameters which may be evaluated before and after the intervention. Their scope is to determine whether a specific intervention registered the anticipated immediate effects, to supervise how such effects are maintained in time or, upon the change of environment (detention vs. freedom), to allow that such measures of impact are examined related to future relapse. Beech and colab. (2007) state that there is a range of important criteria to be met, when performing studies related to the efficiency of some treatment programs for sexual abusers:
1.aleatory repartition in groups, which minimises the pre- existent differences between the group of treatment and that of control,
2.use of different research method, although no procedure is concluding individually, the cumulative effect being important,
3.use of risk, for equivalent repartition of criminals in lots,
4.use of treatments with proven efficiency (4).
Ternowski (2004) speaks about the existence of three approaches in assessing the efficiency of the programs of treatment provided to sexual abusers, each having relevant strong and weak points (5). The first approach involves the analysis based on large lots of criminals, the second is represented by meta-analytic studies and the third involves the measurement of changes registered on the level of subjects on dynamic variables, considered to be related to relapse.
The capacity of an evaluation to detect the effects of treatment depends on the magnitude of results, the size of pattern and the basic relapse rates (percentages of relapse). Due to low basic rates, it is difficult to determine significant effects of treatment, in the absence of large lots of subjects or of some effects of high magnitude, related to treatment. Ternowski states that, under normal conditions, the statistically significant effects are not expected. He exemplifies, presenting the case of treatment which reduces the relapse by 40% and which has an experimental lot of 200 subjects and one of control of 200. This has only a chance of 50% to discover an effect of treatment, if the basic rate of relapse is of 15. The remedy for researchers could be increasing the size of the pattern, the follow-up period (a 10-year period would be efficient, but not economical) or basic rates, by considering the informal, non-official percentages of relapse (5). Marshall and Barbare state that the actual relapse rates are 2.5 times higher than the official ones, thus the solution would be to multiply the real data by 2.5 and we may obtain a rather high rate of start, meant to prove the efficiency of programs (6).
Leaving from the model of creating some efficient programs for criminals, focused on risk, need and responsivity, Looman and colab. (2005) identifies the following factors, related to the capacity of subjects to benefit from treatment: psychopathy, motivation, denying, minimizing, hostility, intellectual operation, deviant sexual excitation, criminal history (7).
Serin and Kennedy (7) propose the TRRG pattern and define motivation and opening for treatment as „probability that an individual enters, continues a treatment and adopts a specific strategy of treatment”. The factors included in the pattern are: capacity to be influenced, motivation, compliance, answer to treatment and earning obtained pursuant to. The areas mentioned by TRRG pattern as being important are: acknowledgement of the problem, perspective over the benefits brought by the participation to treatment, external support, conduct within the treatment, denying, rigidity, ability to apply knowledge and skills in observable contexts (7).The highest degree of overall relapse was encountered on criminals not completing the program, due to moderate, high or very high relapse rate. The overall relapse rate, both for those who completed, and for those not completing the program, was high (69% arrested for committing a new crime and 66% convicted and imprisoned). However, in general the specialised literature indicates higher rates of abandoning the treatment in case of sexual criminals than of other categories of clients (between19-35%).
The researches indicate that those who abandon or are withdrawn from treatments register higher relapse rates than those who complete the treatments (8).
Stalans (2004) synthesizes the characteristics frequently noticed on those who waive the treatment, and these seem to be: deviant, marking and long term sexuality, (paraphilia and many sexual crimes which involve or not touching), defensiveness related to deviant sexual preferences, lack of fundamental knowledge related to human sexuality, presence of obsessive thoughts, sexual abuse in childhood, psychopathy, denying committing the fact, lack of a stable relation, instable occupational history, lack of education (8).
Friendship and Thorton (2001) performs a research over 1.900 sexual criminals, released in 1992 and
1993. The follow-up period is of 4 years, and the relapse rate for a new sexual crime is of 5% (6).
Motiuk (1996) who followed for 3 years 210 sexual treated abusers noticed a reduction by 50% of the relapse risk in their case (9).
Mander and colab. (1996) performed a longitudinal study concerning the evaluation of a program for sexual abusers carried out at Hiland Mountain Correctional Centre between 1987- 1995 (10). In this respect, the authors compare 4 lots of subjects: 411 criminals following at least a part of treatment, 74 subjects who wanted to participate to treatment but who were excluded from program (control lot of motivated criminals), 86 criminals who wanted to take part in the treatment and 100 criminals convicted for other kinds of crimes. The statistic procedure used to analyse the data related to relapse is called „surviving analysis” and it was proposed by Marques and colab. (10). The procedure considers the different periods of time when the individuals are free in the community pursuant to serving the conviction, considering that they enjoy different opportunities of relapse. The technique presented involves a surviving curve when the groups may be compared. The most efficient treatment methods are attached to the longest period of surviving in the community in the absence of relapse. In terms of the results obtained, the research proves that the treatment seems to operate for certain criminals by reducing the relapse incidence for sexual crimes or by extending at least the period of time spent in freedom before committing a new crime. In what concerns the group who benefited from treatment, it is registered a significant positive correlation between the length of the period of time when an individual benefited from treatment and the length of the duration of him being in the community (before committing a new crime).
Beyond the static exigencies, with variables situated between the favourable and non-significant limits of a successful intervention of treatment, the common thread of conclusion shows that the factors stimulated in different kinds of treatment, regardless their nature and diversity, are able to provide benefits to the participants to treatment.
REFERENCES
1. Harkins L, Beech AR. Examining the impact of mixing child molesters and rapists in group-based cognitive-behavioral treatment for sexual offenders. International Journal of Offenders Therapy and Comparative Criminology 2007;10(20): 1-15.
2. Marshall WL, Marshall LE, Serran GA. Strategies in the Treatment of
Paraphilias: A Critical Review. Annual Review of Sex Research 2006;17: 62-180.
3. Perkins D, Hammond S, Coles D, Bishopp D. Review of Sex Offender Treatment Programmes. High Security Psychiatric Services Commissioning Board 1998; 2-23.
4. Beech AR, Bourgon G, Hanson RK et al. Sexual Offender Treatment Outcome Research: CODC Guidelines for Evaluation, Part 1. Introduction and overview, Collaborative Outcome Data Comitee, 2007. Available on-line. http://www.publicsafety.gc.ca, cited on january 2013.
5. Ternowski DR. Sex offender treatment: an evaluation of the Stave Lake Correctional Center Program. unpublished dissertation. Simon Fraser University, 2004.
6. Friendship C, Thorton D. Sexual reconviction for sexual offenders discharged from prison in England and Wales, implications for evaluating and tretament. The Center for Crime and Justice Studies 2001;41: 285-292.
7. Looman I, Dickie I, Abracen J. Responsivity issues in the treatment of sexual offenders, Trauma. Violence and Abuse, 2005;6(4): 330-353.
8. Stalans J.L. Adult sex offenders on community supervision: a review of recent assessment strategies and treatment. Criminal Justice and Behavior 2004; 31:564-608.
9. Motiuk L, Brown S. Factors related to recidivism among released federal sex offenders. Ottawa: Correctional Service of Canada, Research Division, Report R 49, 1996.
10. Mander AM, Atrops ME, Barnes AR, Munafo R. Sex Offender Treatment Program: Initial Recidivism Study. Alaska Department of Corretions and Alaska Justice Statistical Analysis Unit, 1996. Available on-line. http://www.alaskadepartmentofcorrections.com, cited on december 2012.
11. Sawyer S.P., Pettman P.J. Do clients retain treatment concepts? An assessment of post tratment adjustment of adult sex offenders. Sexual Offender Treatment 2006;1: 20-37.
12. Zgoba C.M. Variations in the recidivism of treated and non-treated sexual offenders in New Jersey: an examination of three time frames. unpublished dissertation. The State University of New-Jersey, unpublished doctoral thesis, 2004.
13. Hanson RK, Broom I, Stephenson M. Evaluating Community Sex Offender treatment Programs: A 12-Year Follow – Up of 724 Offenders. Canadian Journal of Behavioural Science 2004;36(2): 87-98.
14. Barnoski R. Sex offender sentencing in Washington State: who participates in the prison treatment program? Olympia: Washington State Institute for Public Policy, 2006. Available on-line. http://www.wsipp.wa.gov, cited on december 2012.
15. Marques JK, Wiederanders M, Day DM, Nelson C, Van Ommeren A. Effects of a relapse prevention program on sexual recidivism: Final Results from California’s Sex Offender Treatment and Evaluation Project (SOTEP). Sexual Abuse: A Journal of Research and Treatment 2005;17(1): 79-107.
16. Seager JA, Jellicoe D, Dhaliwal GK. Refusers, dropouts and completers: measuring sex offender treatment efficacy. International Journal of Offender Therapy and Comparative Criminology 2004;48: 600-612.
17. Illecas SR, Genoves VG. Efficacy of a psychological treatment for sex offenders. Psicothema 2008;20(1): 4-9.
18. Zgoba KM, Simon LMJ. Recidivism rates of sexual offenders up to 7 years later: does treatment matter? Criminal Justice Review 2005;30(2): 155-173.
19. Reitzel LR, Carbonell JL. The Effectiveness of Sexual Offender Treatment for Juvenile as Measured by Recidivism: A Meta-analysis.
Sex Abuse 2006;18: 401 421.
***


