ACUTE AND TRANSIENT PSYCHOTIC DISORDERS AND PARANOID SCHIZOPHRENIA – A COMPARATIVE PILOT STUDY
Abstract
Introduction: The current diagnosis of acute and transient psychotic disorders represents and intermediate station of the long way of the defining and understanding of these nosological entities. This is due to the small number of studies that have been conducted on this topic up to the present moment. This way we presently have so little data available on these “atypical psychosis”. Since their first definition under different heterogeneous forms, they have been considered to be distinct from the major “typical” psychoses – schizophrenia and affective disorders. Comparative studies with the “typical” psychoses have contributed to a better crystallization of the short and transient psychotic disorders. Objectives: The analysis of some socio-biographic and functional aspects of a sample of subjects with a acute and transient psychotic disorder diagnosis as compared to a sample of paranoid schizophrenia subjects. Method: We have selected two samples comprising 41 subjects; the first sample with acute and transient psychotic disorder (ATPD) and the second with paranoid schizophrenia. We have analyzed: the age at onset, educational level, professional and marital status both at onset and after 5 years of evolution. Also, all the subjects have been assessed using the GAF Scale (Global Assessment of Functioning) at the end of the study period. Results: Even if the subjects with ATPD experience a later onset than those with paranoid schizophrenia, the difference is not significant, but we have found significant differences regarding educational and professional status at the end of the study period, both in favour of the ATPD diagnosis. We have also surprisingly found statistically insignificant differences regarding the marital status and the GAF score at the end of the study period. The mean GAF score for the first sample was of 74.17 and for the second sample the mean GAF was 69.27. Conclusions: The differences between the two nosological entities in terms of the socio-biographic and functional aspects analyzed by this study are not all statistically significant.
INTRODUCTION
Psychotic disorders with an acute onset, dramatic and polymorphic symptoms and rapid resolution have been described in different countries and in different psychiatric schools. They have been called cycloid psychosis, “bouffées delirantes”, psychogenic psychoses or good outcome schizophrenia, depending on the geographic area where they were described. Currently we find them in the ICD 10 WHO in the category Acute and transient psychotic disorders and in the DSM IV classified as acute psychotic disorder (1.2). Through the emergence of this new diagnosis category the specialists have tried to integrate the diverse national concepts that have been defining so far this nosological entity. This way, the previous studies on these nosological entities have been based on regional concepts of definition and of denomination. Currently there is a limited amount of studies that explore the new diagnostic and denomination classification of this psychopathological area. So far, little is known on the clinical aspects, the precipitating factors, the longitudinal prognosis, the etiology, the biology and the genetics of acute and transient psychotic disorders.
Ever since their definition under different names,
they have been considered nosological entities different from schizophrenia and affective disorders (the typical psychoses). When reported to schizophrenia, they have been considered to have a better course in terms of the clinical and social functioning. (3) Social functioning is an important feature of the longitudinal assessment of psychoses. There have been several attempts to define social functioning and to establish the aspects that best define it. Overall, social functioning represents the way a person carries out its social roles, meaning an individual succeeds to go to work, has a family and a group of friends he can relate to.
In this study we analyze socio-biographic aspects (age at onset and educational level) and social functioning aspects (professional and marital status) in sample of subjects with ATPD compared to a sample of paranoid schizophrenia. Subjects have also been assessed using the GAF Scale. All subjects have had an average of 5 years of catamnesis.
MATERIALAND METHODS
We have selected subjects that were admitted for the first time in Timisoara Psychiatric Clinic between
2005 and 2008 with ATPD – first sample and paranoid schizophrenia – second sample. We have established the size of the samples starting and according to the evaluation of the number of subjects with ATPD diagnosis who had their first admission during the mentioned period and who retained this diagnosis during 5 years of evolution.
The other inclusion criteria were:
-First admission in a psychiatric facility between 2005 and
2008 in Timisoara Psychiatric Clinic, for both samples subjects
-Age by the time of the first admission ranged between 18 and 65 years
-Clinical diagnosis according to ICD 10 WHO: for the first
sample – Acute and transient psychotic disorder and for the second sample – Paranoid schizophrenia. These diagnoses had to be stable for the 5 years follow-up period
-Active outpatients of the Mental Health Centre Timisoara and of the psychiatric surgeries in Timisoara
-Subjects participate voluntarily in the study, without any kind of motivation from the researchers
We have excluded subjects with a history of substance abuse or dependence.
Within the two samples we have assessed the following parameters: age at the time of the admission, educational level, professional and marital status at onset and after five years of follow-up, GAF Score (Global Assessment of Functioning) at the end of the study period.
We have applied the GAF Scale in order to assess the social functioning of the subjects in both samples. This is a widely used scale that helps psychiatrists to appreciate the global functioning of a subject. GAF is a numerical scale (0-100) that correlates the functioning level of the subject with the severity of his clinical symptoms (DSM- IV-TR, 2000).
Data has been obtained from the analysis of the subject’s medical records and from the discussions with the patients and their doctors. We have acquired both quantitative and qualitative data.
We have used the Mann Whitney non-parametric comparison test and the χ2 test for comparing the frequencies. We have also calculated the descriptive statistic (means, frequencies, percentage).
RESULTS
Two samples have been investigated: one comprising 41 subjects diagnosed with acute and transient psychotic disorder and the other also comprising 41 subjects diagnosed with paranoid schizophrenia.
The average age at onset for the ATPD sample was of
29.34 yrs (std.dev. = 8.7yrs), having a minimum age at onset of 18 yrs and a maximum of 50 yrs.
The average age at onset for the Paranoid schizophrenia
sample was of 27.54 yrs (std.dev. = 7.47 yrs), having a minimum age at onset of 18 yrs and a maximum of 46.
The application of the difference of means test does not
show a statistically significant difference (p=0.319>0.05). The ATPD sample comprises 22 females (53.6%) and 19
males (46.4%). The Paranoid schizophrenia sample comprises 23 females (56.1%) and 18 males (43.9%).
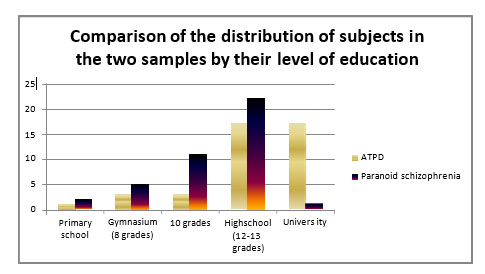
Figure 1. Comparison between educational levels in the two samples
The χ2 test indicates the existence of a statistically significant difference (χ = 31.41, p = 0.0009) between the number of subjects who have attended university from the ATPD sample (17 subjects – 41.5%) and the subjects from
the paranoid schizophrenia sample (1 subjects, 2.4%). In the ATPD sample there are significantly more individuals with a higher degree of education than those pertaining tothe paranoid schizophrenia sample.
The difference we have found cannot be explained only by the existence of an average of two years earlier onset of the subjects in the paranoid schizophrenia sample compared to the ATPD sample. One other possible explanation could be that schizophrenia prodromal symptoms appear long before the onset and can influence the educational performance of the subjects.
The mean GAF Score for the ATPD sample is 74.17 (std.dev. = 11.37), with a minimum score of 56 and a maximum of 95.
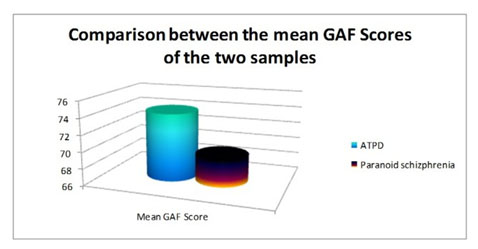
Figure 2. Comparison between average GAF scores in the two samples
The mean GAF Score for the Paranoid Schizophrenia sample is 69.27 (std.dev. = 9.35), with a minimum score of 50 and a maximum of 90.
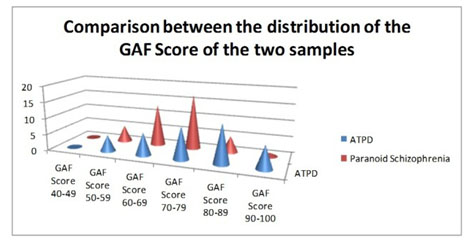
Figure 3. Comparison between the distribution of the
GAF scores of the analyzed samples
A similar distribution of the samples based on the GAF scores can be observed. The Mann-Whitney test does not indicate any significant differences between the two samples regarding the average of the GAF scores (U =
633.5, Z = -1.92, p = 0.055>0.05), although it should be noted that the value of p is close to the statistically significant threshold (p <= 0.05). It is possible that the lack of statistical significance is due to the small number of subjects.
It can be observed that most subjects with ATPD have remained married since the onset; only a small proportion of the unmarried were able to marry after the onset of the disease, and two subjects who were unmarried at the onset got married and also divorced during the period between the onset and the assessment.
Most subjects with paranoid schizophrenia were not married at the onset of the disease and retained their marital status at the assessment time. Only one subject who was widowed at the onset managed to marry during the course of the illness. Three subjects with schizophrenia were divorced at the time of the assessment: one had been divorced since the onset of the illness, another got married and divorced also after the onset and the third got married before the onset and got divorced before the assessment. Overall, we observed a similar trend of the evolution of the two samples in terms of their marital status: unmarried patients rarely manage to get married after the onset of the disease, but most of the patients that got married before the onset did not change their marital status afterwards.
A small amount of the patients with acute and transient psychotic disorder who were unemployed before illness onset were able to work afterwards. The majority of those who were unemployed at onset retained their professional status during the course of the illness and got retired. It can be observed that a large part (80%) of the subjects who were working before the onset also continued to work afterwards.
Out of the 26 subjects with schizophrenia who were working before the onset of disease, only 2 (7.7%) have continued to work afterwards. Also, subjects with schizophrenia who were unemployed at onset remained unemployed or retired.
By comparing the situation we can remark that schizophrenia has a much more strong influence on the work capacity of the subjects than acute and transient psychotic disorder. Thus, schizophrenia is a powerfully disabling disease.
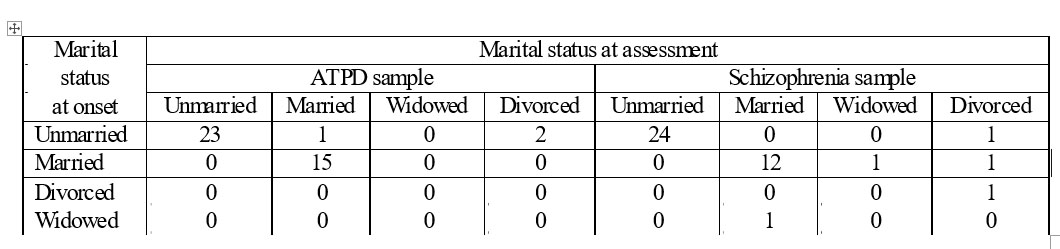
able 1. Marital status at onset and at the end of follow-up of the two samples
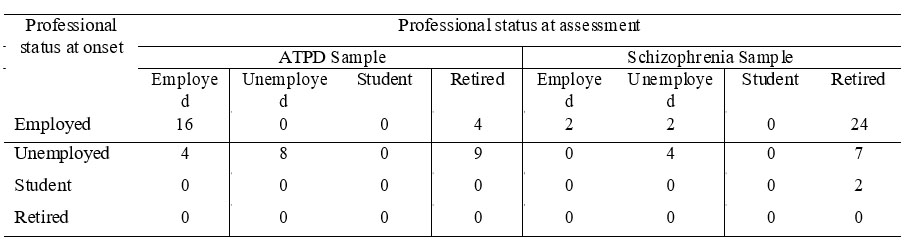
Table 2. Professional status at the onset and at the end of follow-up of the two samples
DISCUSSIONS
Although subjects from the acute and transient psychotic disorder sample had an younger age at onset than the ones from the paranoid schizophrenia sample, the differences were not statistically significant, something that contradicts the existing references up to date of this topic (1984; Tsuang et al, 1995; Hafner and an der Heiden, 1997; Hafner et al., 1998) (4,5,6,7). However, there have been studies which found the age of onset to be approximately equal to or even lower in those with acute and transient psychotic disorder, but it has been considered that it was a methodological artefact (HASBAP Study) (8).
Age of onset for schizophrenia is typically considered to range between 20 to 30 years. It is known that paranoid schizophrenia has a relatively delayed onset compared to the other clinical forms (9, 10, 11, 12).
Acute and transient psychotic disorders can occur at any age, the peak frequency is around the 3rd decade of life. Women have a younger age of onset. (3, 8)
In this study we have found a significant difference in terms of the large number of university graduates from the sample of acute and transient psychotic disorder compared to a sample of paranoid schizophrenia. This could be explained by the earlier onset of schizophrenia (approximately 2 years) compared to the acute and transient psychotic disorder. The pre-morbid functioning of the subjects with schizophrenia should also be considered and also the fact that the prodromal symptoms of schizophrenia tend to occur long before the proper onset and could influence the educational performance of the subjects (13).
If we consider the diagnosis systems and criteria (ICD 10), social functioning should return to the level anterior to the psychotic episode In the case of the acute psychoses sample, it is to be noted that this cannot be supported by the GAF values for a significant proportion of subjects after 5 years of evolution. Many studies have reported a small minority of Acute and Transient Psychotic Disorder patients with unfavourable outcome states, including severely impairments of global functioning.
However the differences are mentioned as significant in almost all of the studies between subjects with schizophrenia and acute and transient psychotic disorder in terms of global functioning. (8)
Subjects from the first sample had a higher GAF score, but the difference was not statistically significant, although it is possible that the lack of statistical significance is due to the small number of cases. The value of the GAF for the first sample corresponds to a very weak difficulty in social, occupational and educational functioning in terms of social functioning. From a clinical point of view these scores correspond to the existence of some transient symptoms which if are present are interpreted as normal reactions to psychosocial stressors. This value is similar to that mentioned by Jorgensen in
1995 at 8 years of evolution, or by the same author in 1997 after 1 year of evolution (an average value of 70) (14, 15). In the sample with paranoid schizophrenia the mean GAF value corresponds to the upper limit of the interval that could be translated functionally and clinically by a mild difficulty in social, occupational and educational functioning and the existence of some mild clinical symptoms.
It should however be mentioned that we only included for this study patients diagnosed with the paranoid form of schizophrenia, which is the form considered to have the best prognostic of all forms of schizophrenia.
Overall, we have observed a similar course for both samples in terms of their marital status: after the onset of the disease, unmarried patients seldom succeed to get married, yet the majority of the ones who got married before the onset of the mental illness keep their marital status unchanged. We found no significant differences regarding the number of married or unmarried patients in the two samples either at the onset or at the end of this study.
Regarding the marital status of the subjects in both samples, we have had a small number of married subjects, both at the study baseline and at the end. When considering this aspect we need to keep in mind that we did not take into account any other long-term heterosexual relationship (except for marriage), condition that would have perhaps lead to a greater number of people in both samples who were under this circumstance.
Whereas, for the subjects with schizophrenia may again come into question the problem of a pre-morbid lack of social interaction that could be related to some personality features (16, 17, 18), for the subjects with acute and transient psychotic disorders we should not neglect the large number of individuals who hold an academic degree. The time invested in the achievement of a university degree could determine a delay in getting married, something which occurs more and more in today’s society.
Furthermore, we need to stress out the role of the stigmatizing of the psychiatric patient when trying to establish close relationships. This issue has been mentioned by the majority of the subjects from both samples and was considered by them to be the main reason of failure to achieve marriage. Previous studies have shown that most of the subjects with acute and transient psychotic disorder have long-term heterosexual relationships in a proportion similar to the normal population (8).
As regards the effect on the professional life, it is noticeable that paranoid schizophrenia subjects present a significant deterioration of their professional status. Most of the subjects from this sample, who have been working at the onset, have become retired due to this illness by the end of the follow-up period. Their retirement occurred after only five years of illness course. The differences between the two samples are significant regarding the number of subjects who remained employed up to the end of the study. Therefore, we have found a better professional status for the subjects with acute and transient psychotic disorder.
Ever since it was first described, schizophrenia has been considered a disabling disease affecting both professional and social roles. The results of our study match with this initial vision of schizophrenia, mainly regarding professional status. Almost all patients who had been working before the schizophrenic onset had become beneficiaries of social aid and assistance and no one of the unemployed managed to work after the onset. At this point we also need to take into account that psychiatric patients encounter higher difficulty in finding a job compared to the mentally healthy individuals. Due to this fact, individuals with a psychiatric diagnosis tend to obtain a disability pension in order to avoid the negative consequences of the unemployment status. The short duration of the psychotic episodes for the subjects with acute and transient psychotic disorder seems not to have a disabling impact on their professional status and only a small percentage of them seek a disability pension. As most of the studies have found, the number of paranoid schizophrenia subjects who receive a disability pension is significantly higher than the proportion of subjects with acute and transient psychotic disorder. (15, 19).
CONCLUSIONS
Considering the small number of subjects in the two samples, we have only found statistically significant differences regarding educational and professional status both in favor of the acute and transient psychotic disorders sample. The stigma of being a psychiatric patient seems to be equally affecting both types of pathology in the achievement of a legal marriage in our society. This equality is not to be found in the other studies of this kind.
However, this study has not found any statistically significant differences regarding the age of onset and the GAF Score. We believe that this is because we have only included in the schizophrenia sample only patients with the paranoid form and with only five years of evolution.
We may conclude that, within our study, the differences between the subjects with paranoid schizophrenia and acute and transient psychotic disorder regarding socio-biographic aspects and social functioning are not as obvious as the ones mentioned in the other studies on this topic.
New prospective studies, that include a larger number of subjects, will be needed in order to better characterize and define the acute and transient psychotic disorders.
CONFLICTS OF INTERESTS
The authors do not have any conflicts of interests to report.
REFERENCES
1.***ICD-10.Clasificarea tulburărilor mintale şi comportamentale, simptomatologie şi diagnostic clinic. Bucureşti: Editura All, 1998.
2.*** Diagnostic and Statistical Manual of Mental Disorders, 4th edition. Text Revision (DSM-IV-TR). Washington D.C: American Psychiatric Association, 2000.
3.Romosan F, Romosan RS. Tulburările psihotice acute şi tranzitorii. In: Ienciu M, Romosan F, Lazarescu M (eds). Schizofrenia şi tulburările de spectru. Timişoara: Editura Brumar, 2012.
4.Loranger AW. Sex difference in age at onset of schizophrenia. Arch Gen Psychiat 1984;41:157-161.
5.Tsuang MT, Tohen M and Zahner GEP. Textbook in Psychiatric Epidemiology. New York: Wiley-Liss, 1995.
6.Hafner H and an der Heiden W. Epidemiology of schizophrenia. Can J Psychiyt 1997;42: 139-151.
7.Hafner H, an der Heiden W, Behrens S et al. Causes and consequences of the gender difference in age at onset of schizophrenia. Schizophrenia Bull 1998;24: 99-113.
8.Marneros A, Pillmann F. Frequency and sociobiographic characterstics of acute and transient psychotic disorders (ATPD) and brief psychoses (BP). In: Marneros A, Pillman F. Acute and transient psychosis. Cambridge: University Press,2004,71-102.
9.Suvisaari J, Perala J, Saarni SI at al. The Epidemiology and Descriptive and Predictive Validity of DSM-IV Delusional Disorder and Subtypes of Schizophrenia. Clinical Schizophrenia and Related Psychoses 2009;2(4): 289-97.
10.Kendler K.S and Walsh D. Schizophreniform disorder, delusional disorder and psychotic disorder not otherwise specified: clinical features, outcome and familial psychopathology. Acta Psychiatr Scand 1995;91: 370–8.
11.McGlashan TM. Psychosis treatment prior to psychosis onset : Ethical issues – Schizophr Res 2001;51: 47-54.
12.Fenton WS, McGlashan TH. Natural history of schizophrenia subtypes. I. Longitudinal study of paranoid, hebephrenic, and undifferentiated schizophrenia. Arch Gen Psychiatry 1991;48(11): 969–77.
13.Olin SC, Mednick SA, Cannon T et al. School teacher ratings predictive of psychiatric outcome 25 years later. Brit J Psychiat (Suppl) 1998;172: 7-13.
14.Jorgensen P. Comparative outcome of first-admission patients with delusional beliefs. Eur Psychiat 1995;10: 276-281.
15.Jorgensen P, Bennedsen B, Christensen J and Hyllested A. Acute and transient psychotic disorder: a 1-year follow-up study. Acta Psychiatr Scand 1997;96: 150-154.
16.Watt DC and Syulecka TK. The effect of sex, marriage and age at first admission on the hospitalization of schizophrenics during 2 years following discharge. Psychol Med 1979;9: 529-539.
17.Riecher-Rossler A, Fatchenheuer B, Loffler W, Maurer K and Hafner H. Is age of onset in schizophrenia influenced by marital status? Some remarks on the difficulties and pitfalls in the systematic testing of a ‘simple’ question. Soc Psych Psych Epid 1992;27: 122-128.
18.Thara R and Srinivisan TN Outcome of marriage in schizophrenia. Soc Psych Psych Epid 1997;32: 416-420.
19.Marneros A, Pillmann F. The long-term outcome. In: Marneros A, Pillman F. Acute and transient psychosis. Cambridge: University Press,
2004, 143-156.
***


