ASPERGER SYNDROME: CONVERGENCE WITH OTHER PSYCHIATRIC DISORDERS
Abstract
Introduction: The phenotypical characteristics of adolescents with Asperger syndrome can often be mistaken for symptoms of other psyhciatric disorders. Moreover, the Asperger syndrome is frequently associated with other psychiatric pathologies, making it difficult to establish an early diagnosis and to start the appropriate therapy. Given the high level of functioning that these patients have, their addressability in specialized services is further delayed. Objectives: To identify the specific traits of Asperger's syndrome, according to ICD-10, in a sample of patients exhibiting polymorphic symptoms; to establish the usefulness of using the “Childhood Asperger Syndrome Test” (CAST) as an aid for the clinical investigation and to evaluate the general functioning level of these patients. Materials and methods: This observational clinical study has been performed on 16 subjects, aged 12 to 18, who were admitted in the Child and Adolescent Psychiatry Department, “Prof. Dr. Al Obregia” Hospital”, between 2009 and 2012. All these patients had symptoms such as social withdrawal, depressive mood, solitary lifestyle, educational maladjustment, narrow interests. A senior psychiatrist set the diagnoses according to ICD-10 criteria. The scales that were used were CAST and CGAS. The results were analyzed using SPSS 16.0. Results: 50% of the subjects met the ICD-10 Asperger Syndrome criteria, whereas 87.5% had a CAST score above the cutoff for this pathology. There was no statistically significant difference between the CAST scores of patients with Asperger Syndromes, and the ones without this pathology. Their average functioning level was between 51 and 60, according to CGAS. All the subjects associated at least one more psychiatric disorder. Conclusions: There are three factors that can make the early diagnosis of Asperger Syndrome difficult: the symptoms that are characteristic for the disorder, but that are also met in other psychiatric pathologies, the occurrence of comorbidities and the level of general functioning.
INTRODUCTION
The Asperger Syndrome is classified under the umbrella of autism spectrum disorders, together with atypical autism and infantile autism. A social communication deficit, a narrow range of activities and interests and no significant language or cognitive development impairment characterize it. The estimated worldwide prevalence of the syndrome is 3/10.000 (1, 2). Even though the diagnosis is possible starting from 36 months, the average age at which the patients are brought to the doctor is 11 years (3). In spite of the fact that patients suffering from this pathology are often met with social difficulties (e.g incapacity of having a conversation, a lack of establishing or maintaining friendship relationships, empathy difficulties and problematic adjustment to transitions, their coming to the doctor’s is often delayed, especially because of the patient’s IQ, which is frequently over 70, and because of the normal development of expressive speech (4).
Another frequently encountered problem in the diagnosis of Asperger Syndrome is the high number of a s s o c i a t e d c o m o r b i d i t i e s . T h e m o s t c o m m o n manifestations that have been reported to coexist with this pathology are depression, bipolar disease, anxiety disorders, obsessive compulsive disorder, tics and disruptive and aggressive behavior (5)(6). Even thought the schizophrenia diagnosis represents an exclusion criterion for the Asperger Syndrome diagnosis, studies have shown that these two pathologies have a common pattern of social-cognitive functioning and a similar deficit of social abilities. Furthermore, it has been proven that patients with Asperger Syndrome and patients with schizophrenia score similar results at tasks regarding The Theory of Mind (“The Eyes Task”), Emotions perception (“The Point-Light Motion Displays”) and the Social Judgments (“The Abbreviated Social Task”) (7).
The differential diagnosis of Asperger Syndrome is firstly done with other pervasive developmental disorders, from which it varies through the presence of expressive language and an almost normal cognitive d e v e l o p m e n t , a n d s e c o n d l y w i t h o t h e r neurodevelopmental disorders that have the same behavioral traits. While the first step of this differential diagnosis will be totally eliminated by officially grouping all autism spectrum disorders in one category in DSM-V, there are still a number of pathologies that must be taken into account before setting the diagnosis of Asperger Syndrome (i.e. schizophrenia, schizotypal and schizoid personality disorders, developmental learning disability of the right hemisphere, social-emotional learning disabilities, the multiple complex developmental disorder, a d u l t a t t e n t i o n – d e f i c i t h y p e r a c t i v i t y d i s o r d e r, obsessive–compulsive disorder, depression, semantic pragmatic disorder, etc. (8, 9) ). Given the clinical resemblances with other pathologies, as well as the great number of comorbidities, the diagnosis of Asperger Syndrome becomes a challenge for the psychiatric clinician, associated with a potential negative impact of a postponed, scarce or omitted medical treatment that comes from a misdiagnosis. The international guidelines recommend using ICD-10 or DSM-IV-TR criteria in the clinical evaluation, together with applying one of the specific screening and diagnostic tools. The tests that can be used as adjuvant measures are “Gilliam Asperger’s Disorder Scale”, “Asperger Syndrome Diagnostic Scale”, “Krug Asperger’s Disorder Index” “Autism Spectrum Screening Questionnaire”, “Childhood Asperger Syndrome Test” (10, 11, 12, 13, 14).
The main aim of the study is to identify the specific traits of Asperger’s syndrome, according to ICD- 10, in a sample of patients exhibiting polymorphic symptoms. Other secondary endpoints are: to establish the usefulness of using the “Childhood Asperger Syndrome Test” (CAST) as an aid for the clinical investigation, to identify the psychiatric comorbidities of Asperger Syndrome and to evaluate the general functioning level of these patients.
MATERIALAND METHODS
The sample consisted of 16 patients recruited
from the Child and Adolescent Psychiatry Department, Psychiatry Hospital “Prof. Dr. Al. Obregia”, Bucharest, Romania. Data were collected prospectively (2009 to 2012) upon first admittance to the hospital. Children participating in the study were 14 males and 2 females, aged between 9 and 18. (mean age= 14.69, SD= 2.77). At the time of recruitment, each parent signed an informed consent form for their children’s participation in this study. The subjects were enrolled in this study based on the presence of at least four of the following symptoms:
-Social isolation
-Depressed mood
-Aggressive outbursts
-Lack of friendships and solitary lifestyle
-Social inadequacy
-School maladjustment or dropout
-Affective flattening
-Peculiar and narrow interests
Other clinical features were observed in our sample but were not considered as mandatory eligibility criteria: auto-aggressive behaviour, agitation, echolalia, atypical prosody, anhedonia, delusional ideas, compulsive overeating, sleep disturbances. Diagnoses were generated by experienced clinicians using the ICD 10 criteria. Social functioning was assessed using the Children’s Global Assessment Scale. A number of diagnostic and cognitive measures were used in the initial evaluation, depending on which symptoms were most prominent (e.g. Beck Depression Inventory, CY-BOCS, ADOS-G, ADHD-RS).
Childhood Asperger Syndrome Test (CAST) was administered to all subjects in the study, in order to screen for behavioural core symptoms of AD. The CAST is a parent-rating questionnaire with 37 items (yes/no questions), out of which 31 are relevant for the AD score and 6 are controls, examining the general development. Exceeding a lower-limit cutoff score of 15 is considered to predict AD. Designed as a screening test, rather than a diagnostic instrument, a comprehensive assessment was carried out in order to confirm the syndrome.
The statistical software package SPSS 16.0 has been used to conduct data analysis. We performed descriptive statistics (measures of central tendency, measures of variability), Fisher’s exact test, Spearman’s Rank Correlation test and inferential nonparametric tests for significance (i.e. Mann-Whitney test). The level of significance was established at 0.05 (two-sided).
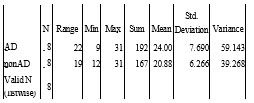
Table 1. CAST scores
RESULTS
The clinical assessment based on ICD-10 criteria revealed the following primary diagnoses: Asperger’s Disorder (50%, n=8), Schizophrenia (18.75%, n=3), Severe Depressive Episode (12.5%, n=2), Acute Psychotic Episode (12.5%, n=2), Mixed Dissociative Disorder (6.25%, n=1). Further on, subjects were divided in two groups (AD and nonAD) according to the presence or absence of AD diagnosis. Table 1 displays the descriptive statistics of CAST scores in each group.
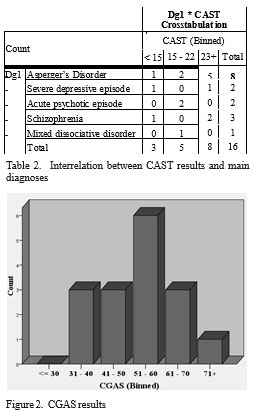
Out of all the participants, 13 (81.25%) subjects exceeded the cutoff, scoring above 15 points, with almost half of them (n=6) falling between 20 and 25 points (Figure 1). Of all the subjects with CAST scores above the cutoff (n=13) only 7 of them received a diagnosis of Asperger Disorder. Only 1 participant was diagnosed with AD but rating below the limit value of 15 points (CAST = 9 points) (Table 2). A Mann-Whitney U-test was performed to assess whether the CAST scores were significantly different between the AD and nonAD groups. The computed two-tailed p-value was 0.316, which indicates that there is no statistically significant difference between the groups regarding CAST scores. Applying Fisher’s exact test, there is no significant difference in under cut-off / above cut-off ratio between AD and nonAD groups.
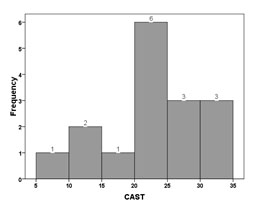
Figure 1. CAST scores – Frequency Histogram
All the 31 relevant-questions included in the CAST were separately analyzed, both in AD and nonAD groups. Elevated frequency of positive responses (Yes/ No depending on the question) in 3 items were observed in both groups: (Question 10- A:No) “Does s/he find it easy to interact with other children?”; (Question 17- A:No) “Does s/he enjoy joking around?”; (Question 27- A:No) “Does s/he make normal eye-contact?”. Three questions revealed statistically significant difference (p<0.01, Fisher’s exact test) between the groups, with AD group scoring positive more frequently: (Question 9) “Does s/he like to do things over and over again,in the same way all the time?” (Question 19) “Does s/he appear to have an unusual memory for details?” and (Question 29) “Is his/her social behaviour very one-sided andalways on his/her own terms?”
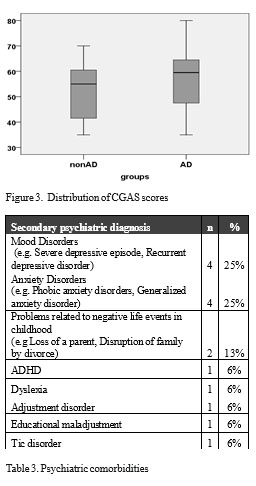
Analysis of ratings from CGAS showed a mean general functioning score of 54.81 (min=35, max=80, SD= 12.875), with the highest percentage of subjects (37.5%) falling in the interval of 51 to 60 (“Variable functioning with sporadic difficulties or symptoms in several but not all social areas”)(Figure 2). A comparative distribution of the subjects’ CGAS scores is shown in Figure 3. In order to confirm that AD subjects have higher CGAS scores, as observed in our sample, we performed a Mann-Whitney U test. There is no statistically significant difference (U=27.00, p= 0.598) between AD and nonAD groups regarding their CGAS ratings. As expected, we found no meaningful correlation between CGAS and CAST scores (Spearman’s rho= 0.266, 2-tailed p=0.319).
Furthermore, an analysis of the frequency and the pattern of other psychiatric comorbidities was conducted. All of the subjects of our sample have at least one other psychiatric comorbidity. Among these, the most common are: affective disorders(25%) and anxiety disorders(25%). Table 3 displays the co-existing psychiatric conditions in our subjects.
DISCUSSIONS
In adolescents, the characteristic symptoms of Asperger Syndrome can be found in the clinical manifestations of other psychiatric disorders. In a homogenous group of participants that were clinically characterized by social withdrawal, lack of friends, solitary lifestyle, narrow interests range, depressive mood, social inadequacy, 50% meet the international criteria for Asperger Syndrome diagnosis. The other half of the study’s patients have been diagnosed with the following pathologies: schizophrenia, depressive episodes, acute psychotic episodes, dissociative disorders. Schizophrenia represents one of the main entities of this syndrome’s differential diagnosis. Studies show that patients with these pathologies share a similar pattern of social difficulties (15). The research conducted on the relationship between the Asperger Syndrome and depressive disorders have shown that patients with Asperger Syndrome have greater depression rates than healthy individuals, with a higher incidence of chronic unhappiness and loneliness (16). Another recent study has reported that 70% of the young adults with Asperger Syndrome have had at least one major depressive episode and that 50% of them are suffering from a recurrent depressive disorder (17). Therefore, the pathologies that make up the differential diagnosis entities for Asperger Syndrome overlap with its comorbidities, which makes setting the diagnosis even harder. The main comorbidities that were identified in the present group were mood disorders (i.e. severe depressive episode, recurrent depressive disorder), anxiety disorders (i.e. phobic anxiety disorders, generalized anxiety disorder), problems related to negative life events in childhood (i.e. loss of a parent, disruption of family by divorce), ADHD, dyslexia, adjustment disorder, educational maladjustment and tic disorders. These match the comorbidities reported so far by other studies. The most frequent associated psychiatric conditions that the patients of the present study have had were affective disorders (25%) and anxiety disorders (25%).
When the diagnosis of Asperger Syndrome is presented according to ICD-10 criteria, the Childhood Asperger Syndrome Test represents a useful instrument in confirming the diagnosis, having a diagnosis rate of 87.25% among the patients confirmed by ICD-10. It seems, however, that this test can also return a great number of false positives. In the group presented in this study, 75% of the patients that did not meet the ICD-10 criteria for Asperger Syndrome scored higher than the cut- off limit of this scale. Moreover, the CAST scores did not vary significantly among the range of pathologies. These results confirm once again that the symptoms of Asperger Syndrome can be present in a wide variety of psychiatric conditions, and that an accurate diagnosis requires the simultaneous usage of ICD-10/ DSM-IV-TR criteria and standardized scales for diagnosis and screening.
Even if the social interaction deficits of Asperger patients may lead to their isolation, given their real deficits in carrying on conversations, in establishing friendships, in scholar and work place collectivity integration, their general functioning level is an average one. In the studies group, this level is situated at the middle of the CGAS scale (51-60 points), most of the subjects displaying a variable functioning with sporadic difficulties or symptoms in several but not all social areas. Though the clinical severity of the syndrome is, probably, negatively correlated with the functioning level, the total number of specific symptoms grouped as a total CAST score has not proven to have a proportional relationship with the functioning CGAS score.
CONCLUSIONS
When faced with an adolescent who exhibits clinical traits such as social isolation, depressed mood, aggressive outbursts, lack of friendships and solitary lifestyle, social inadequacy, school maladjustment or dropout, affective flattening, peculiar and narrow interests, the Asperger Syndrome is one of the main diagnostic suspicions, together with schizophrenia and depressive episodes. Another problem of diagnosing this syndrome is the high occurrence of comorbidities, especially mood and anxiety disorders. The general level of social functioning of Asperger Syndrome patients is, most of the times, an average one. This can delay their coming to a specialized consult, thus having a negative impact upon the early intervention, which is necessary in Asperger Syndrome.
REFERENCES
1. Fombone E. Epidemiology of autistic disorder and other pervasive developmental disorders. J Clin Psychiatry 2005;66(10): 3-8.
2. Rondeau E, Klein LS, Masse A, Bodeau N, Cohen D, Guilé JM. Is Pervasive Developmental Disorder Not Otherwise Specified Less Stable Than Autistic Disorder? A Meta-Analysis. J Autism Dev Disord 2011;41(9): 1267-76.
3. Scott FJ, Baron-Cohen S, Bolton P, Brayne C. The CAST (Childhood Asperger Syndrome Test): Preliminary development of a UK screen for mainstream primary-school age children. Autism 2002;6: 9-31.
4. Balfe M, Tantam D. A descriptive social and health profile of a community sample of adults and adolescents with Asperger syndrome. BMC Research Notes 2010;3: 300.
5. Mazzone L, Ruta L, Reale L. Psychiatric comorbidities in asperger syndrome and high functioning autism: diagnostic challenges. Annals of General Psychiatry 2012;11: 16.
6. Meyer JA, Mundy PC, Van Hecke AW, Durocher JS. Social attribution processes and comorbid psychiatric symptoms in children with Asperger syndrome. Autism 2006;10(4): 383–402.
7. Couture SM, Penn DL, Losh M, Adolphs R, Hurley R, Piven J. Comparison of social cognitive functioning in schizophrenia and high functioning autism: more convergence than divergence. Psychol Med
2010;40(4): 569–579.
8. Szatmari P. Differential Diagnosis of Asperger Disorder. Autism 1998; 61-76.
9. Fitzgerald M, Corvin A. Diagnosis and differential diagnosis of
Asperger syndrome. Adv Psychiatr Treat 2001;7: 310-318.
10. McClintock JM, Fraser J. Diagnostic instruments for autism spectrum disorder. New Zeeland: New Zealand Guidelines Group, 2011,1-27.
11. Campbell JM. Diagnostic Assessment of Asperger’s Disorder: A Review of Five Third-Party Rating Scales. J Autism Dev Disord 2005;35(1): 25-35.
12. Matson JL. Current status of differential diagnosis for children with autism spectrum disorders. Res Dev Disabil 2007;28(2): 109–118.
13. Ehlers S, Gillberg C, Wing L. A Screening Questionnaire for Asperger Syndrome and Other High-Functioning Autism Spectrum Disorders in School Age Children. J Autism Dev Disord 1999;29(2): 129- 141.
14. Williams J, Scott F, Stott S, et al.The CAST (Childhood Asperger
Syndrome Test) Test accuracy. Autism 2005;9(1): 45-68.
15. Raja M, Azzoni A. Thought disorder in Asperger syndrome and schizophrenia: issues in the differential diagnosis. A series of case reports. World J Biol Psychiatry 2009;10(4): 944-52.
16. Green J, Gilchrist A, Burton D, Cox A. Social and Psychiatric Functioning in Adolescents with Asperger Syndrome Compared with Conduct Disorder. J Autism Dev Disord 2000; 30(4): 279–293.
17. Lugnegård T, Hallerbäck MU, Gillberg C. Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res Dev Disabil 2011;32(5): 1910–1917.
***


