VIOLENCE AND SUICIDE RISK INCIDENCE IN THE PENITENTIARY SYSTEM
Abstract
The Romanian penitentiary system is interested in the evolution of suicide cases quantified as violent acts, appeared in the establishments they manage. In the penitentiary establishments from Romania, in 2012, the suicide registered an alarming increase by 120% in comparison to prior years (2010-2011). The state, through the penitentiary institution, is liable for the well-being of the individuals convicted to execute a punishment. From the data supplied by the Medical Directorate, it results that during the period of January 1st 2009 – December 31st 2012, 51 cases of suicide were registered in 24 penitentiary units from Romania. Simultaneously, the self-aggression increases (3.3%) and the percentage of aggression over the staff decreases (from 80 cases in 2010-2011 to 13 cases in 2012). The self-aggressive acts are committed in a percentage of 76.24% by individuals convicted for committing violent offences. The hetero-aggressive acts and the suicide attempts follow the same track: their number decreased significantly in 2011 and presented an increase in 2012, without reaching the values from 2010. The suicide attempts are associated to violent crimes and are frequent to the individuals from maximum safety, closed regime or custody on remand.
The suicide became a problem of public health in the 21st century, the suicide being the 11th death cause in the world and the second death cause among the individuals aged between 25-34 years, 30-40% of youth aged between 9 and 18 registering at least one suicide attempt. (1) The reduction of suicide rate became an important objective globally. According to OMS, from a test group of 400 million individuals from 25 countries, it is estimated that the average rate of suicide ranges between 18 and 100.000 inhabitants. Globally, the suicide rates range from over 25 to 100.000 inhabitants in Scandinavia, Switzerland, Germany, Austria, East-European countries and Japan, up to 10 to 100.000 in Spain, Italy, Ireland, Egypt, Netherlands. (1)
The repartition on sex reveals the predominance among men in committing suicide, although the attempts are much more frequent among women. The methods differ as well, women selecting suicide methods which do not lead to sure death (ingestion of pills, cutting the veins), whereas men choose tough methods such as hanging, shooting in the head or height falling. (1)
The men-women suicide report, in Romania, is between 4.5:1. The suicide risk seems to be reduced by marriage and by the presence of children, who operate even as protective factors. (1)
The suicide average in Romania is of 13 on every 100.000 inhabitants, little under the European average. The Hungarians, Finnish and French people are in the top of suicide in Europe, on the other side, being encountered the British and Italian people. (2)
As for the preferred method of suicide, Romanian selected hanging (80%), poisoning (9%) and drowning (3%). (2). The statistics of the National Institute of Legal Medicine “Mina Minovici” show that the profile of Romanian suicide is the following: man, aged under 45, unhappy financially or disappointed in love. (2)
Around 90% of the individuals committing suicide could be diagnosed with a psychiatric emotional t r o u b l e ( m a j o r d e p r e s s i o n , b i p o l a r t r o u b l e , schizoaffective trouble) (Carroll-Ghosh & colab., 2003; Maris & colab., 2000; Moscicki 1999; Simon 2004 apud. Gold, 2006). (3)
Between 18-38% of the individuals committing suicide attempts to take their lives in the past (Jacobs et al.
1999; Maris & colab., 2000; Moscicki 1999; Skogman & colab., 2004; Zahl & Hawton 2004, apud. Gold, 2006). (3) The individuals committing suicide register a
higher rate of alcohol addiction comparatively to women committing suicide (Kung & colab., 2003; apud. Gold,
2006), the percentage being of 81.8% for men respectively 18.2% for women (Garlow 2002 apud Evans & Farberow 2003). (3, 4).
The patients with personality troubles register a suicide risk 7 times higher than general population. And among the patients committing suicide, 30%-40% are diagnosed with personality problems (Simon 2004, apud Gold 2006). (3)
The diagnosis of a trouble from cluster B, mainly borderline, is associated to high rates of suicide, ranging between 4% and 9.5% (Kung et al. 2003, apud Gold,
2006). (3)
The anti-social personality trouble is more frequently diagnosed on men comparatively to women, between 3-5% on men and 1% of women meeting the diagnosis criteria (Phillips, 2003 apud. Oquendo & colab.,2006). (5)
In the specialised literature, the imprisoned suicide is presented as generally being young, alone, on his first conviction privative of freedom for a non-violet offence, intoxicated, presenting a history of substance abuse; in his case, death is caused by hanging with bed linen while being closed in an isolated cell, during the first 24 hours of his imprisonment (Hayes 1983, 1989, apud Metyner & Hayes, 2006). (6)
New York State Department of Correctional (Metyner & Hayes, 2006) confirms this profile by psychological autopsies on 40 cases of offenders committing suicide between 1993 and 2001. All convicts who committed suicide benefited from mental health services during the imprisonment. The factors associated to the suicide risk are: substance abuse, suicide attempt in the past and psychiatric treatment before imprisonment, receiving recent bad news, recent disciplinary deviation and manifestation of agitation or anxiety. (6) Most of them are offenders convicted for violent crimes and have been assigned schizophrenia diagnosis (Kovasznay & colab., 2004, apud Metyner & Hayes, 2006). (6)
He & colab. (2001, apud. Metyner & Hayes, 2006) determined that 64% of the individuals committing suicide had at least one suicide attempt in prison and 2/3 had psychiatric diagnosis (affective trouble 64%, personality trouble 56% and psychotic trouble 44%.) (6, 7)
Patterson & Hughes (2000, apud. Metyner & Hayes, 2006) identified the following characteristics: alone in the cell (67%), imprisoned for sexual crimes (40.6%), the method selected is hanging (81.2%), they manifested a suicide conduct in the past (63%), and they had recently followed a psychiatric treatment at nursery (13%). Their case is also associated to improper evaluation (cancel the appointments, do not fill in the questionnaires, there is no file in the archives, 62.5%), lack of answer to recent threats or gestures (25%), case charge (72%). (6)
The profile of suicide risk of convicts in Romania (Pripp & Ţogoie, 2009) associates suicide to the following elements: men, old persons, bachelor, in custody on remand, risking punishments privative of freedom on long term/for life, who committed violent crimes (murder, rape), presenting mental troubles (with actual symptoms of anxiety, depression, anguish etc.) and existence of suicide attempts in the past. The suicide was mainly committed by hanging during the first weeks of imprisonment, most frequently on Saturday and under the influence of precipitating factors (negative family events, anniversaries, events preceding the appearance in court, perspective of a too long conviction or getting close to the term of liberation from penitentiary of the convicts who served a long term conviction). (8)
In the penitentiary environment, the actual suicide risk is difficult to identify. Although death pursuant to suicide increased in prison, however the number of individuals committing suicide is significantly lower to those identified as presenting a suicide risk. In other words, thinking of suicide does not necessarily entail to the actual act. Thus, the practitioner in mental health is liable to evaluate the intensity of suicide thoughts of convict and the risk of such acts. In addition, the practitioner has to manage to distinguish between the individuals imprisoned presenting a suicide risk and those who, by their conduct, leave the impression that they want to commit suicide or simulate suicide attempts or they self-mutilate. A rigorous evaluation gives the possibility to distinguish the suicide conduct from simulation or self- mutilation, as distinct clinical syndromes, each of such manifestations involving methods of intervention and different treatment plans. Unfortunately, the demarcation between these three categories is often unclear, which renders difficulty in the task of the practitioner who has to pass an opinion related to the existence of the suicide risk. In most of the cases, the diagnosis of a mental disease is not determined as aggravating factor, but we have to consider the clinical emotional troubles (major depression, bipolar trouble, schizoaffective trouble). The identification of prior attempts of suicide is not an easy task, but it is very important to know such data, as the risk of another attempt increases in the following period. (9)
On the actuality of violence consumed in the penitentiary establishments from Romania, our novelties are neither good nor bad. Related to the year 2012, the issues are gradated: the favourable ones refer to massive reduction of aggressions on staff whereas the worrying ones refer to the amplitude of violence of hetero and self- aggressive manifestations, of attempts and suicide acts. The referential exemplification is represented by suicide, phenomenon that registered an increase by 120% in 2012, comparatively to prior years (2010-2011).
The penitentiary system collects all data related to human dysfunctional phenomena: hetero and self- aggression, attempts and acts of suicide and aggressions over staff. The annual complete centralizing situation (as of 2010) represents a rich source of information and allows periodical comparisons between negative events.
The average custodial effective represents the annual average number of individuals in custody of penitentiary system (and it does not reflect the entire effective).
The share of convicts involved in self-aggressive actions is represented by individuals that committed violent crimes. For instance: in 2012, the 799 convicts imprisoned for violent crimes (329 for robbery, 310 for aggravated theft, 87 for rape and 73 for murder) represent 76.24% of the 1.048 self-aggressive individuals. Thus, the self-aggression actions are frequent on maximum safe closed regime or on individuals imprisoned under remand.
The suicide attempts are associated to violent crimes and are frequent on individuals from prisons with maximum safety, closed regime, or imprisoned under demand. We do not have enough data on such conducts meant to clear us of the self-destructive or the simulating character.
The hetero-aggressive actions represent violent forms of manifestations and are correlated to the violence the criminals committed. As the number of individuals involved in altercations increases, the consequences are higher: serious injuries, even the death of victims, and the material losses are difficult to recover.
The hetero-aggressive acts and suicide attempts follow the same track: decrease significantly in 2011 and present an increase in 2012, without reaching the values from 2010
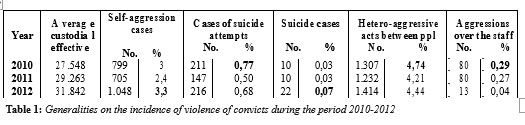
The only phenomenon following a favourable evolution, in the sense of reducing it, is that of the aggressions directed against the staff. An explanation may be that the staff is better trained and the communication with the convicts does not leave place to interpretations, discussions etc.
The completed suicide registered an exponential increase. The suicide committed by imprisoned individuals causes troubles to his family and friends, preoccupies the public, while the state, by the penitentiary institution, is liable for the well-being of those convicted to serve a punishment.
Comparatively to other negative phenomena encountered among the penitentiary population, the suicide is not a quantitative reference. However the dramatic nature of the suicidal act, the consequences thereof are very high.
Based on the data supplied by the Medical
Directorate, it results that, during the period of January 1st 2009 – December 31st 2012, 51 suicide cases were registered, in 24 penitentiary units. If during the period 2005-2008, the suicide acts of convicts ranged between 6 and 13 cases, during the last 4 years, 2009-2012, we speak about minimum 9 and maximum 22, as mentioned in the Chart 1.
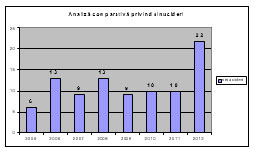
Chart 1: Comparative situation of convicts’ suicide, during the period 2005-2012
Comparative analysis of suicide
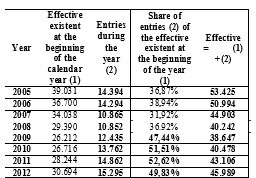
Table 2: Evolution of penitentiary population, during the period 2005-2012
The most accurate figure for reporting the statistic data is that of the effective ran. The calculation needs multiple and periodical data from subordinated units and becomes relevant on long terms, such as the calendar year.
The effective ran during a calendar year (passed through the penitentiary system) is calculated by totalizing the existent effective (number of convicts in the
penitentiary on 1st January) of the entries during the year (individuals imprisoned during the year to serve the convictions). The gross data was supplied periodically (monthly) by the department of Safety of Detention and Penitentiary Regime.
From the perspective of primary statistics it is obvious the progressive increase of the number of convicts entered every year since 2009 (with values between 47% and 52% of the volume existent at the beginning of the year). However, this is the year 2009 when the first modification of suicide conduct become obvious. If we add, to the quantitative aspect, that of increase of violence of crimes for which imprisonment is ruled, the ascendant evolution of dysfunctional human phenomena in penitentiary is perfectly justified.
In a classification of violence incidence, the hetero-aggressive actions are in the top, followed closely by self- aggressions, on a significant distance are located the suicide attempts, followed by the aggression over the staff, whereas the suicide, as supreme form of destruction is on the lower line of hierarchy. The number of seriously risky situations is lower, in comparison to the forms, we could call them of release of fury in the form of self-aggressions or actions directed towards the other convicts – hitting a convict rather than an employee or suppression of his own life has less serious consequences. This could represent an explanation for the increase share of self-aggressive acts. Longitudinally, the autolytic acts present a progressive increase: from a share of 50, in 2005-2006, it tripled during the period of 2007-2009, so that within the last 3 years, to increase 8-10 times opposite to the first period analysed. An explanation may as well be that the law of execution of punishments enforced the legislative act at the end of the year 2006 which provides many liberties on the ground of extremely high prior restrictions. About the massive numerical increase of autolytic acts from the period of
2010-2012, the background of the problem may be represented by the violence of crimes committed.
As of 2010, we notice the doubling and even tripling of the number of suicide attempts. It is possible that the penitentiary staff (guard officer, general medicine physician, medical nurse) evaluating the violent events for fear of risking the occurrence of a suicide, is tempted to extend the sphere of suicide attempts by the elements of simulation, para-simulation, self-aggressions. Mainly considering that since 2009, the specific program of psycho-social assistance and prevention of suicide risk is applicable
The analysis of attempts’ incidence in the comparison to the completed suicide indicates the following pattern: the increase of suicide is associated to the reduction of the number of attempts and reverse, with a single exception in the year 2012, when both phenomena registered a high level.
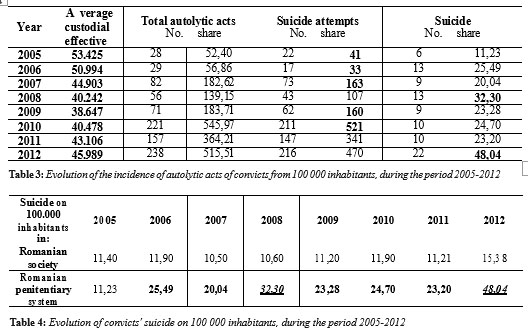
For reporting with the same measurement unit, respectively, the number of cases on 100.000 inhabitants, we present the suicide in Romania comparatively to that of Romanian penitentiary system. The data related to Romanian population is taken over from Eurostat 2011 statistics (10).
During the entire period analysed, 2005-2012, the data of the National Institute of Statistics refer to: 25.630.252 Romanians.
If on the level of population, the suicide rate is maintained within rather constant limits – with a reduction between 2007 and 2008 – the situation is different related to the penitentiary population, where fluctuations are much gradated and highly oscillating.
The suicide cases, in the last 4 years, took place within 24 penitentiaries:
-15 units (88%) of 17 establishments with closed regime and maximum safety
-3 units (75%) of 4 Penitentiaries for Underage and Youth,
– 2 units (33%) of 6 Penitentiaries – Hospital,
-4 units (25%) of 16 with open and semi-open regime.
G e n e r a l l y, w e r e f e r t o h i g h c a p a c i t y penitentiaries, which:
•provide custody predominantly in restrictive detention:
closed and maximum safety,
•keep in custody between 600 and 1.400 individuals – the convicts are serving long-term convictions (over 15 years) for life for violent crimes or their deviations, which, during the execution of their conviction are so serious, that they need to be passed from easy (open or semi-open) to a
more restrictive regime,
•have limited possibilities of including the convicts in waged labour, activities of social reintegration, volunteering in community (legislative, the restrictive regime is suspended for rendering labours/activities in community, as well as by the numerical conditions imposed for forming such groups).
We may conclude that in the penitentiary system, the numerical increase of individuals imprisoned for committing violent actions is directly proportional to violence incidence of conduct manifestations in penitentiaries and, implicitly, to that of suicide.
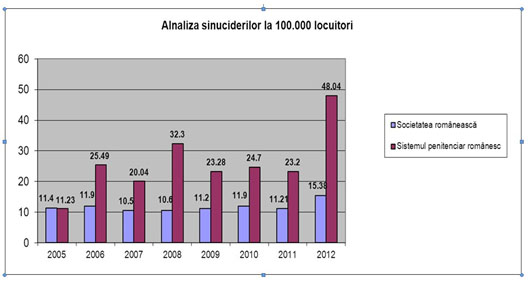
Chart 2: Share of suicide acts of convicts on 100 000 inhabitants, during the period 2005-2012
Analysis of suicide on 100.000 inhabitants
REFERENCES
1.“Ziua mondială de prevenire a suicidului” posted in September 2012. Available on-line.http://www.sanatateatv.ro/10-septembrie-ziua- mondiala-de-prevenirea-a-suicidului. Website, visited on September 2012.
2.“Maghiarii şi ilfovenii în topul sinuciderilor din România” published i n A u g u s t 2 0 1 2 . A v a i l a b l e o n – l i n e . h t t p : / / www.ziare.com/articole/sinucideri+romania+2011, website visited on October 2012.
3. Gold LH. Suicide and gender, in Simon RI, Hales RE. Textbook of suicide assessment and management, The American Psychiatric Publishing, 2006, 77-107.
4. Evans G, Farberow NK. The Encyclopedia of suicide, II-nd ed, Facts on File Inc, New-York, 2003.
5. Oquendo MA, Carballo JJ, Stanleyâ B, Brodsky BS. Personality
disorders, in Simon, R.I., Hales, R.E. Textbook of suicide assessment and management, The American Psychiatric Publishing, 2006, 329 – 47.
6. Metyner JL, Hayes LM. Suicide prevention in jails and prisons, in Simon RI, Hales RE. Textbook of suicide assessment and management, The American Psychiatric Publishing, 2006. 139-59.
7. Pripp C, Ţogoie S. PsychoSocial Program for suicidal risk in jail, Bucharest: National Administration of Penitentiaries, Social Reintegration Directorate, Print&Grafic, Râmnicu Sărat, 2009.
9. Bulgaru-Iliescu D, Costea G, Enache A, Oprea L, Gheorghiu V, Astărăstoae V. Psychiatric forensic expertise: Interdisciplinary approach, Timpul Publishing House, Iaşi, 2013.
1 0 . E u r o s t a t 2 0 1 1 s t a t i s t i c s . A v a i l a b l e o n – l i n e . http://epp.eurostat.ec.europa.eu., website visited on October 2012.
***


